This is another post written by Brooks Walsh, with some editing by Smith.
Ken Grauer, who is truly an ECG guru, also had a hand in the analysis of this ECG. Visit his extremely informative site here: ECG Interpretation
Case
A
teenage male was brought to the ED
with 1 week of a left-sided pleuritic chest pain and cough. He had a modest hypoxia, and a temperature of 99.9. He had no documented cardiac disorders.
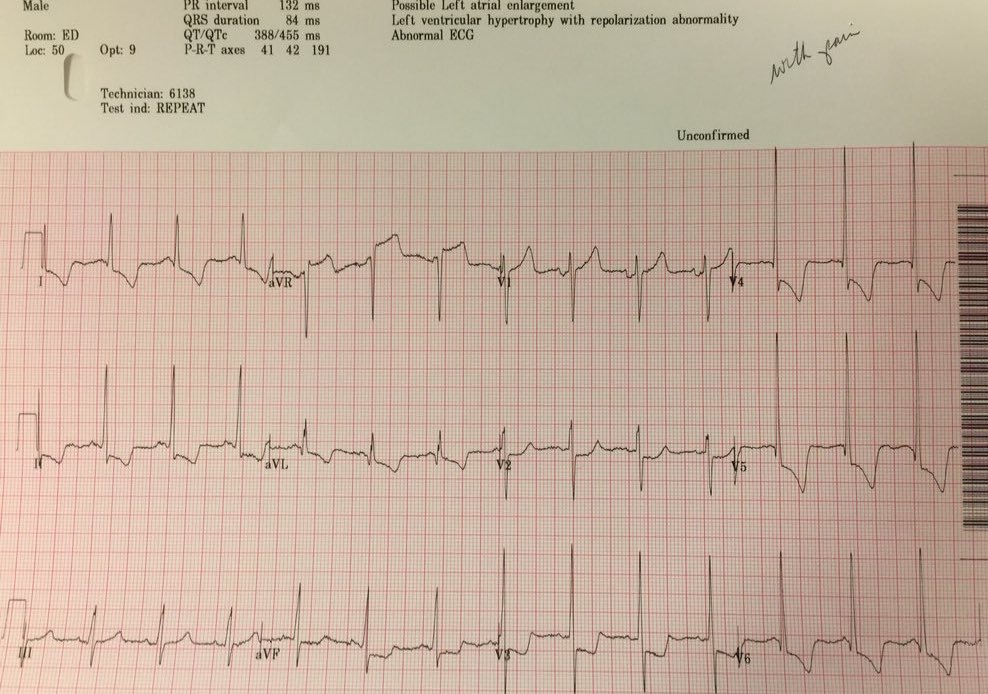
An ECG was obtained:
 |
|
There The R waves in V1 are abnormally tall, There are also deep (though narrow) Q waves in I, aVL, V5, and V6. |
Why does he have these tall R-waves in right precordial leads and Q-waves in lateral leads? Could he have a previous lateral and posterior myocardial infarction (now classified as inferobasal)?
Several conditions can cause the increased R/S in V1:
-
WPW? But no delta waves to suggest WPW.
-
Posterior MI? But young age, and no supportive ST/T changes in V1-V3.
-
(I)RBBB? But no no rSR’ pattern in V1, no deep lateral S waves
-
RVH? But no S waves in I, aVL, or V6, and no right axis deviation or right atrial abnormality
-
Hypertrophic Cardiomyopathy (HOCM) with Septal Hypertrophy – voltage is inadequate
-
Lead Misplacement – checked and ok.
On the other hand, the pattern of a tall R in V1, and deep Q waves in I, aVL, and V5, V6 is classic for Duchenne’s muscular dystrophy (DMD)!
In fact, records revealed that he is known to have Duchenne muscular dystrophy.
The CXR suggested aspiration pneumonitis (± pneumonia), consistent with multiple prior hospitalizations, and explaining the patient’s chest pain.
These ECG features were found in the majority of patients with DMD in the seminal 1968 paper by Slucka:
 |
| From Slucka. Type “a” was most common, seen in 64/106 DMD patients. |
More recent studies (example, example, example, and example)
have shown more variability in the presence of either tall R waves or
deep lateral Q waves in DMD patients. Nonetheless, these “distinctive” features are considered to be classic.
The tall R waves in V1 and the deep lateral Q waves are thought to reflect myocardial fibrosis in the posterobasal and lateral myocardium. Although these changes represent disease progression in the myocardium, they have not been shown to be age-related, perhaps because ECG changes occur quite early in life,
proceeding clinical or echocardiographic signs. Although DMD patients
do develop a progressive and inevitable left ventricular cardiomyopathy,
the classic ECG changes do not seem to be correlated with echo findings (such as reduced EF or increased LV size), or with the presence of dilated cardiomyopathy.
![]()