An 85 year old called 911 for palpitations.
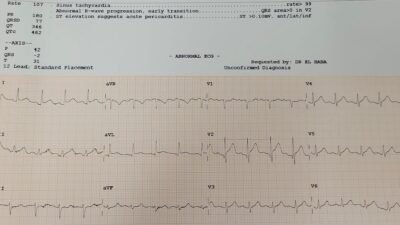
Medics found her with good blood pressure but fast rate and recorded this ECG?

Opinion of Zoll algorithm and medic: junctional tachycardia.
My response: it is NOT junctional tachycardia. There are subtle waves showing that the underlying rhythm is atrial flutter at a rate of 256, with ventricular rate of 128 (2:1 conduction), and the wide complex is due to RBBB/LAFB.
Here I point them out with red arrows:

These are very subtle, but I was convinced.
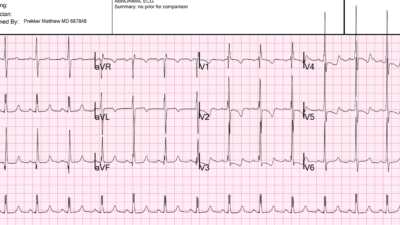
Let’s see if there is a baseline RBBB/LAFB
So I found a Previous ECG, and it indeed shows pre-existing RBBB/LAFB, proving that this is a supraventricular rhythm and NOT VT.

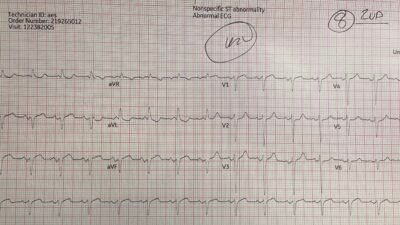
I wanted to show the medic more visible flutter waves, so we recorded an ED ECG with lead II rhythm strip shows flutter waves much more obvious

If you can’t see them, look at Ken’s diagram at the bottom. It is diagnostic of atrial flutter at a rate of 256 with 2:1 conduction and ventricular rate of 128.
What is unusual about this flutter? It is slow! When flutter is slow, suspect an anti-dysrhythmic medication such as flecainide.
Chart review confirmed that she has had this before, been cardioverted before, and is on amiodarone. Importantly, she was also on diltiazem so that the AV node would not be able to conduct at 1:1 if the atrial flutter rate was slowed too much on amiodarone (an atrial rate of 200 could suddenly conduct 1:1 and result in a ventricular rate of 200. This can be very dangerous. See this post.
She was on apixaban for her atria flutter, so cardioversion would be safe.
Very soon thereafter, we performed electrical cardioversion to sinus:

= = =
She felt much better. We discharged her and told her to double her amiodarone dose. Follow up in one week.
======================================
MY Comment, by KEN GRAUER, MD (10/31/2025):
Assessment of regular WCT (Wide-Complex Tachycardia) rhythms is always a challenge — and today’s case presented by Dr. Smith is no exception. I love this case — because it is full of PEARLS on arrhythmia interpretation.
- For clarity in Figure-1 — I’ve reproduced the 1st and 3rd tracing shown in Dr. Smith’s discussion — which are the initial ECG in today’s case, done by the EMS team on their arrival at the scene — and the repeat ECG done on arrival in the ED.
= = =
Among the PEARLS in today’s case include the following:
- The BEST approach to the diagnosis of today’s initial rhythm is not by saying the rhythm is SVT or AFlutter or VT — but instead, to simply describe what we see — which is a Regular WCT rhythm without clear sign of sinus P waves (no upright P wave in lead II) at a rate of ~130/minute.
- This description should immediately prompt our differential diagnosis of 5 entities — each of which needs to be worked through before jumping to a single diagnosis. These 5 entities include #1) VT (Ventricular Tachycardia) until proven otherwise! — vs — an SVT (SupraVentricular Tachycardia) with QRS widening due either to aberrant conduction or preexisting bundle branch block (with the 4 most common regular SVT rhythms to consider being sinus tachycardia — a reentry SVT (AVNRT, AVRT) — Atrial Tachycardia — or Atrial Flutter).
- It is indeed fortunate that Dr. Smith found a previous ECG on today’s patient — because it’s important to appreciate that QRS morphology in ECG #1 is much more suggestive of VT, than of an SVT rhythm. This is because although the predominant R wave in lead V1 with wide terminal S wave in lead V6 and the marked left axis deviation in the frontal plane suggest RBBB/LAHB — there is no terminal S wave in either lead I or aVL — which in the absence of the prior ECG, would have been much more consistent with VT than with a supraventricular rhythm.
- It is also worth a reminder that 7 leads in ECG #1 manifest the automatic truncation of R wave or S wave amplitude at 10 mm, as is common with pre-hospital ECGs in the U.S. (dotted BLUE lines in leads II,III,aVL,aVF; V2,V3,V6). While not important to today’s diagnosis — automatic truncation of pre-hospital ECGs sometimes can make a huge difference in our interpretation! (See My Comment in the June 20, 2020 post).
- Accurate estimation of heart rate in ECG #1 is important for making the rhythm diagnosis. As I emphasize in the November 12, 2019 post — untreated AFlutter will almost always present with a regular rhythm with 2:1 AV conduction and a ventricular rate close to 150/minute (usual range between ~130-170/minute).
- In the 2:30 minute ECG Video below — I review rapid estimation of fast heart rates in a regular tachycardia. I also review how to look for subtle 2:1 atrial activity. What is especially interesting (and insightful) about today’s case is how subtle flutter waves are in ECG #1 — but that they become much more obvious in the repeat ECG. I believe the reason for this is that every-other-flutter-wave that had been hiding within the last last part of the S wave upslope in ECG #1 — moved forward ever so slightly as to now appear just after the QRS in ECG #2 (slanted RED lines now much more evident in leads II,III,aVR and aVF in ECG #2). But my use of calipers — and the strong suggestion of 2:1 atrial activity (as shown in ECG #1 and as illustrated in the ECG Video below) — is what clued me into the diagnosis of AFlutter even before I saw ECG #3.
= = =
Figure-1: Comparison between today’s initial ECG done at the scene by EMS — and the repeat ECG on arrival in the ED.

= = =
ECG VIDEO on today’s case (2:30 minutes) — reviewing use of the Every-other-Beat Method for rapid estimation of fast heart rates — and beginning at 1:05 minutes in the video, How to look for 2:1 flutter waves.