
Here is another case written by Pendell Meyers, a G2 at Stony Brook. As I mentioned before, Pendell will be helping to edit and write the blog
Special thanks to Dr. Atif Farooqi who cracked this
case for me.
Case
A male in his 50s with history of “SVT with
two prior failed ablations” presented for acute onset palpitations and
shortness of breath. He appeared mildly short of breath and diaphoretic, but he
was mentating perfectly, laughing about how many times he had been in this same
situation. His initial automatic BP was 83/51, immediate manual pressure was
98/58.
Before we even get to his ECG, is he
“stable” or “unstable”? This of course depends on your
definitions, prior experience, and various other factors. If you care how the
ACLS guidelines defines “stable vs. unstable”, then prepare yourself
for confusing and contradicting descriptions.
ACLS defines unstable as “a condition in which
vital organ function is acutely impaired or cardiac arrest is ongoing or
imminent.” (1)
Problem #1: Acute vital organ impairment is a
definitively different level of instability compared to imminent or ongoing
cardiac arrest.
An asthma attack may constitute
acute impairment of a vital organ’s function, but clearly does not imply
impending cardiac arrest.
They then give a list of suggested criteria which
satisfy that condition, including terms such as “ischemic chest
discomfort” and “acute heart failure.” (1)
Problem #2: These terms have high interobserver variability
Unless it is the rare and obvious
version of crushing chest pain in a clearly sick patient who is so diaphoretic the electrodes don’t stick, how are we to agree
upon what types of chest symptoms are “ischemic chest discomfort”?
The majority of patients feel some sort of sensation in their chest with any
rapid heart rate. Some insist that is is not pain, but rather
“pressure,” “discomfort,” “throbbing,”
“tightness,” or “fluttering.” When ACLS warns about the patients with “ischemic” chest pain among all those with any chest symptoms, it seems that one is supposed to assume the worst, that the patient’s chest discomfort is indeed ischemic. Similar
confusion exists regarding what constitutes “acute heart failure” in
the setting of tachycardia.
The ACLS dichotomy is therefore both confusing and
oversimplified. It does not account for the spectrum of variability seen in
actual practice, and it does not help the clinician understand when to use electricity vs. less aggressive interventions for a tachydysrhythmia. Immediate electrical cardioversion is necessary when there is an imminent risk of deterioration.
Proposed criteria which satisfy this restricted definition of
unstable are:
- Acutely
altered mental status or obtundation - Overt signs of shock
- Acute
heart failure causing pulmonary edema and severe respiratory distress which
would otherwise require noninvasive or invasive positive pressure ventilation - Sustained
Polymorphic VT
Criteria 1-3 imply immediate risk of airway
compromise, critical hypoperfusion, and/or critical hypoxemia. Additionally,
traditionally first line interventions such as vagal maneuvers or adenosine in
these cases are not feasible and/or risky, as the brief bradycardia or
hypotension induced by these therapies may not be tolerated in the already
tenuous hemodynamic state. In the setting of sustained PMVT, the rhythm itself carries an
inherent risk of immediate deterioration and cardiac arrest, even in the momentary absence of the other criteria above. Polymorphic VT is a slightly more organized
version of VFib and is treated identically, with unsynchronized defibrillation.
A truly unstable adult patient whose instability is
presumed to be caused by a tachydysrhythmia (other than PMVT) should undergo immediate
synchronized cardioversion with 150-200 J under procedural sedation sedation.
Sedation is unnecessary and dangerous if the patient is already obtunded. The
monitor must be checked prior to every synchronized cardioversion to ensure
that the machine is not syncing on the T-wave to avoid R-on-T phenomenon and
rhythm deterioration.
Back to the case:
Here is the patients presenting ECG:
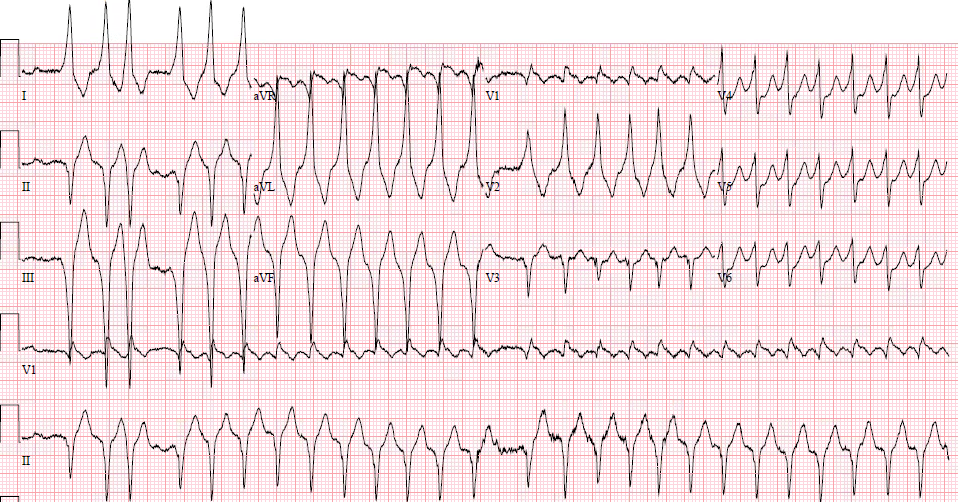 |
| What is your interpretation? |
The first step in interpreting and managing
tachyarrhythmias is classifying it according to two questions:
1) Narrow or Wide
2) Regular or irregular
This produces a limited differential for each category. More
importantly, it offers an immediate empiric management strategy which will be
safe and effective even without knowing the specific rhythm diagnosis within
that category:

Irregular rhythms can be further subdivided into “regularly” irregular or “irregularly” irregular. Irregularly irregular is completely chaotic and unpredictable, and is seen primarily with atrial fibrillation, but also with MAT and polymorphic VT. Regularly irregular occurs with sinus arrhythmia, sinus rhythm with variable AV block, PACs, PVCs, and atrial flutter with variable block.
So what do you do when you’re not sure if the rhythm is regularly or irregularly irregular?
Do not miss a truly irregularly irregular wide complex rhythm, because of the potential harms
of any AV-nodal blockading medications in the setting of preexcited AF.
Therefore if there is uncertainty, the clinician should assume an irregularly
irregular rhythm and proceed accordingly. With that proviso, regularly
irregular QRS complexes usually represent
1) Single regular rhythm with constant or variable AV
block
Examples: atrial flutter with variable block, sinus tachycardia with LBBB and rate-related RBBB, etc
2) Single regular rhythm with frequent premature beats
Examples: sinus rhythm with frequent PACs, sinus tachycardia with LBBB and frequent PVCs, etc
3) Two or more separate and competing
rhythms
Examples: sinus rhythm with interjecting runs of VT or SVT, etc
This
ECG shows a wide complex tachycardia which is overall irregular and has QRS
complexes with differing morphology. Thus, the first consideration should be
atrial fibrillation with WPW (preexcited AF), and this was my first impression.
But there are sections of wide complex regular monomorphic rhythm within the
tracing. AF can never be regular, so this cannot be AF with WPW. So you must
break the ECG up into segments to understand what is happening. Here is the
annotated ECG:
 |
|
There are two separate and consistent QRS morphologies in this ECG. |
The differential for the runs of regular
monomorphic wide complex tachycardia is of course: VT, SVT with conduction
abnormality, all plus or minus hyperkalemia.
There are no features particularly worrisome for hyperkalemia. There are also no features that suggest
obvious VT, such as concordance. If you thought the other distinct QRS
complexes were possibly fusion beats or capture beats, then there should not
have been a break in the rhythm just before them. Fusion/capture beats are
described when one rhythm is constantly present before, during, and after the
beat in question. Instead, this rhythm is repeatedly starting, terminating, and reoccuring. This makes short acting drugs like adenosine useless, because the rhythm will likely resume immediately after adenosine wears off.
Let’s take a closer look:
 |
| In leads I, III, and V2, the QRS complexes marked with a black arrow can be seen to have a distinctly slow upslope, consistent with a delta wave. Thus, these QRS complexes may be supraventricular in origin with a delta wave or may simply be PVCs (in which case they are not delta waves). Either way, it seems as though the QRS complexes marked by arrows are initiating each run of monomorphic wide complex tachycardia. The reason these runs terminate is not exactly clear, but there is possibly an upright P-wave seen just after the last T-wave of each group (marked by red arrows). They do not appear to be retrograde P-waves. |
There is no way to exclude VT based on this ECG,
but presence of single QRS complexes with possible delta waves preceding
regular tachycardia raises the suspicion of a regular reentrant rhythm using a
bypass tract, such as atrioventricular reciprocating tachycardia (AVRT, see below). The beats indicated by black arrows initiate the AVRT, then it continues until something (possibly the atrial activity indicated by red arrows) terminates it, and it starts again.
Refresher on AVRT:
(“Macroreentrant” is a large loop such as in atrial flutter, whereas “microreentrant” is a tiny loop such as seen in intra-nodal reentry in which the entire loop is contained within the AV node)
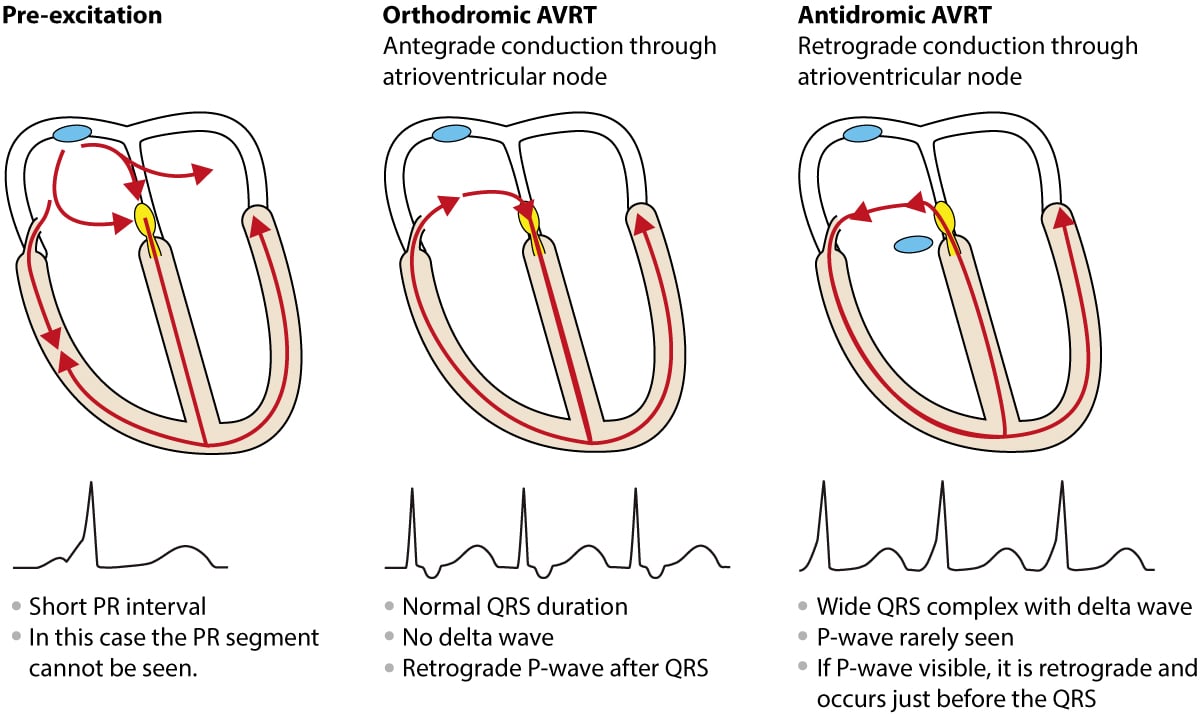
Atrioventricular Reentrant Tachycardia (AVRT) is a
macroreentrant rhythm involving the atria and ventricles, requiring
an abnormal atrioventricular accessory pathway (also known as “bypass
tract,” “Bundle of Kent”) in addition to the AV node. The
accessory pathway may be able to conduct antegradely (from atria to
ventricles), retrogradely (from ventricles to atria), or both, and these
properties may also be transient and fluctuating based on various
conditions.
In sinus rhythm, the AP originates at the SA node
and enters the AV node and the accessory pathway simultaneously (in
parallel). Whereas the AV node normally has slow conduction (causing the
delay between the P-wave and the QRS), the bypass tract does not, and depolarization
through the bypass tract begins first (“preexcitation”). Because the bypass
tract does not connect directly to the specialized conduction system, the
impulse traverses slowly through myocardium. Since slow conduction creates a
wide QRS complex, this results in a wide initial deflection known as a “delta”
wave. When the AP from the AV node transmits down through the conduction
system, it rapidly converges with the AP from the bypass tract. This manifests
as a fusion beat with the initial part of the QRS abnormal (delta wave) and the
latter part appearing more normal.
An appropriately timed premature contraction may
find one pathway refractory while the other is able to accept the premature
impulse. By the time the AP arrives at the other pathway, it has fully
repolarized and can continue the circuit in series. The macro-reentrant loop
may proceed in an orthodromic (anterogradely down the AV node and retrogradely
up the accessory pathway) or antidromic (opposite) fashion. Orthodromic AVRT
activates the ventricles using the intrinsic conduction system, resulting in
QRS morphology identical to the patient’s baseline (unless rate-related BBB is
present). Antidromic AVRT involves the spread of conduction through the
myocardium without using the intrinsic conduction system, resulting in a WCT
which is often indistinguishable from VT.
See this diagram for explanation of the waveforms
created by the presence of the bypass tract:
https://ecgwaves.com/wp-content/uploads/2016/08/AVRT-1.jpg
When AVRT results in a narrow rhythm, it must have
accessed the intrinsic conduction system antegradely (usually via the AV node),
and is termed orthodromic AVRT. When the QRS complex is wide as in this
case, it is either antidromic AVRT (accessing the ventricles via the
bypass tract) or orthodromic with conduction abnormality despite using the
conduction system (BBBs, Non-specific IVCD, hyperK, Na channel blockade).
Case continued
No prior ECG was available, and no prior medical
records were on file. Medics reported they had attempted adenosine 6 and 12 mg
en route with no perceived change in rhythm. The patient was presumed to be
symptomatic from the rhythm, and had concerning vital signs and physical
exam features, but it seemed clear to the providers at that time that he was
not at risk for impending cardiac arrest.
The rhythm was thought at the time to be an
irregularly irregular wide complex rhythm, because the patterns above were not
yet recognized.
Amiodarone infusion was ordered. (If your patient actually has AF with WPW, this could be dangerous! Like adenosine, amiodarone may not be safe in AF with WPW. Its beta blocking effect could result in rhythm deterioration, and it is thus contraindicated in the ACLS and SVT guidelines for any irregular or polymorphic wide complex tachycardia). (1,2)
45 minutes after the infusion was started, the patient became
progressively more hypotensive (~80/40) and less alert despite no change in the
rhythm. He underwent sedation and electrical cardioversion, which immediately
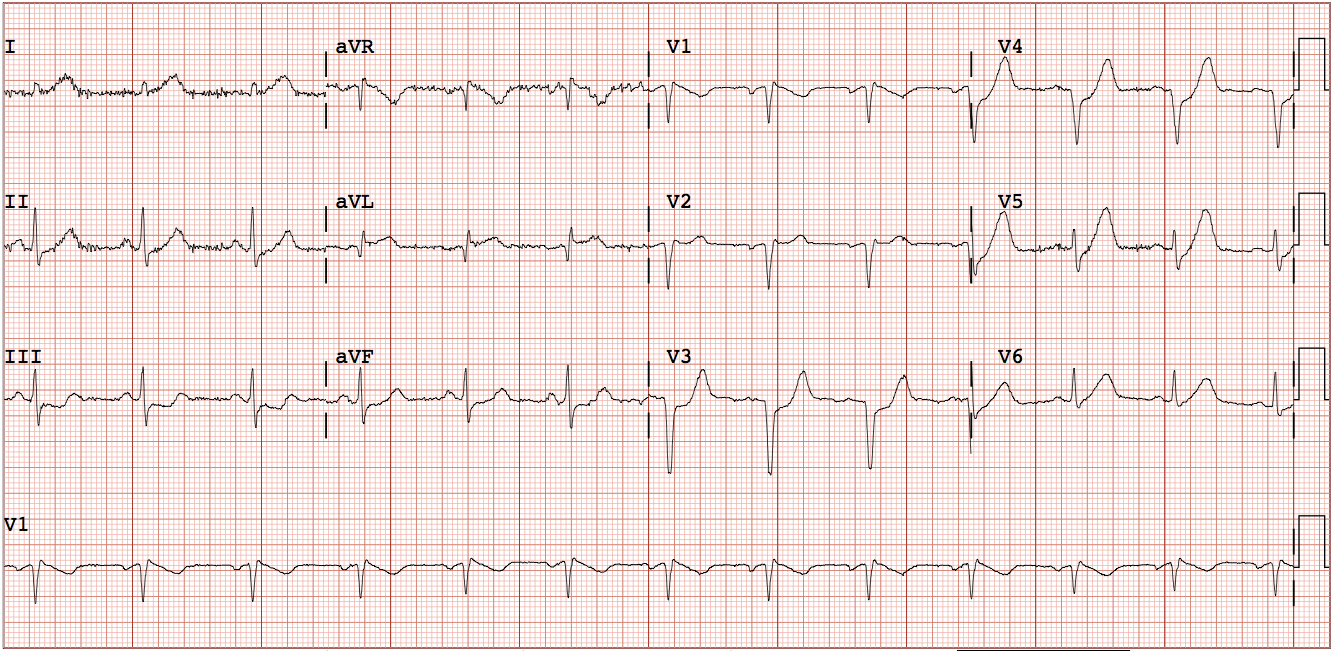
produced this ECG:
 |
|
| Sinus rhythm with distinct delta waves. This further supports the suspicion of intermittent runs of antidromic AVRT. The QRS morphology does not appear to match the singular beats marked by black arrows in the prior ECG.
|
The patient’s mental status and vitals quickly
normalized, and the rhythm did not recur. Normally, cardioversion or short
acting medications would not solve this problem because the recurring rhythm
should simply recur immediately after therapy (this is why longer acting
medications are indicated in this scenario). Amiodarone acts via multiple mechanisms, and could potentially be stopping the initiation of AVRT by preventing PACs or PVCs (labelled by red arrows above). Cardiology was consulted, and the patient was admitted to undergo
an EP study.
Here is the report of the ED study:
“The patient presented to the lab in NSR,
antidromic AVRT was induced with catheter manipulation which degenerated into
AF requiring multiple cardioversions. The patient never stayed in AVRT long
enough to permit full diagnostic maneuvers. There was no retrograde bypass
tract conduction. Mapping of earliest antegrade activation was performed during
atrial pacing, the R posteroseptal area had some early sites but ablation was
unsuccessful. Mapping the MV annulus revealed an early site that resulted in
loss of preexcitation with bumping, when preexcitation returned ablation at
this site resulted in permanent loss of preexcitation at 1.4 seconds into the
first ablation lesion.”
Thus, the patient had apparently successful
ablation of a left posteroseptal bypass tract.
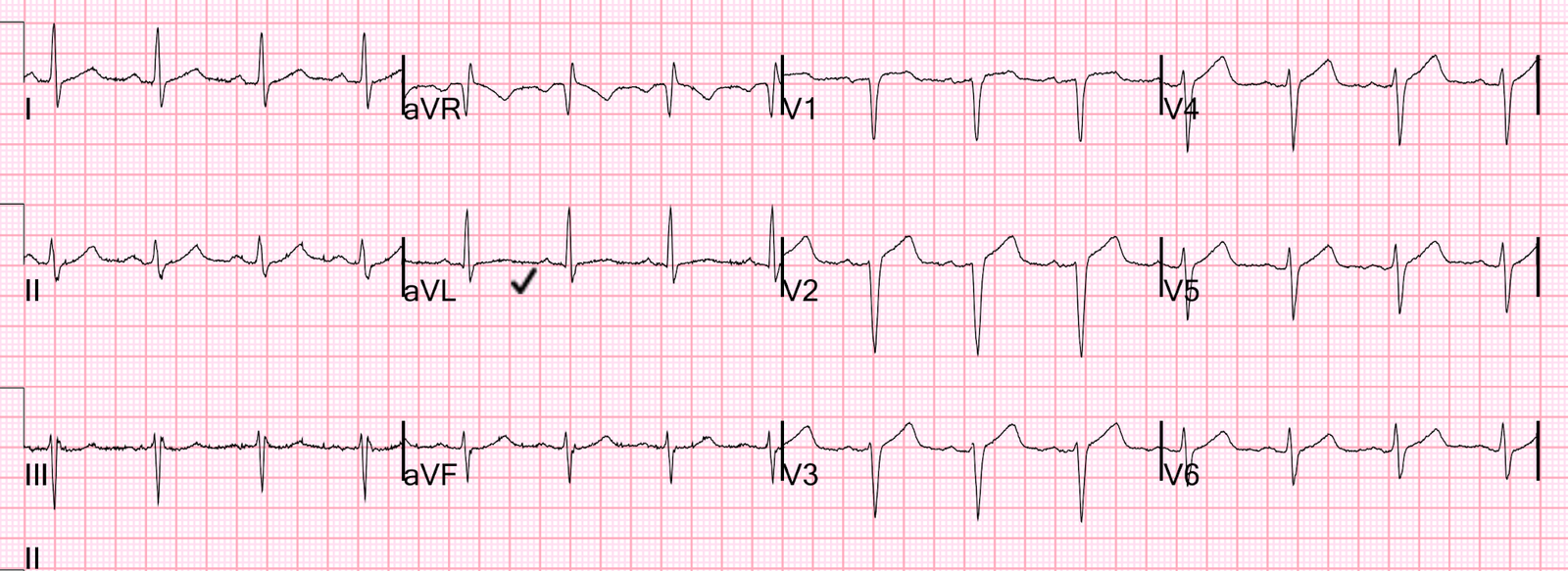
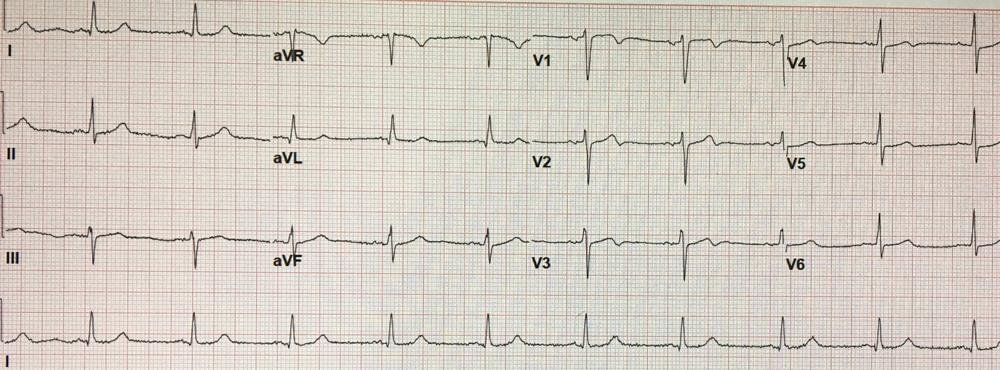
Here is his post-procedure ECG:
 |
|
|
He has been free of palpitations and arrhythmias
for over 1 year.
Learning Points:
- Stable
vs. unstable is not well defined by the current ACLS guidelines, but the
clinician should be able to recognize the signs of impending deterioration and
change management accordingly - When a
wide complex rhythm is not perfectly regular and also not irregularly
irregular, one should consider AV blocks, premature beats, or multiple
competing/alternating rhythms, while keeping in mind the risks of missing an
irregularly irregular wide complex tachycardia - Antidromic
AVRT is a rare condition which causes regular wide complex monomorphic
tachycardia that can be indistinguishable from VT or hyperkalemia-accompanied
arrhythmias
References:
{kind=link}