History: This woman in her 20’s (age) with history of
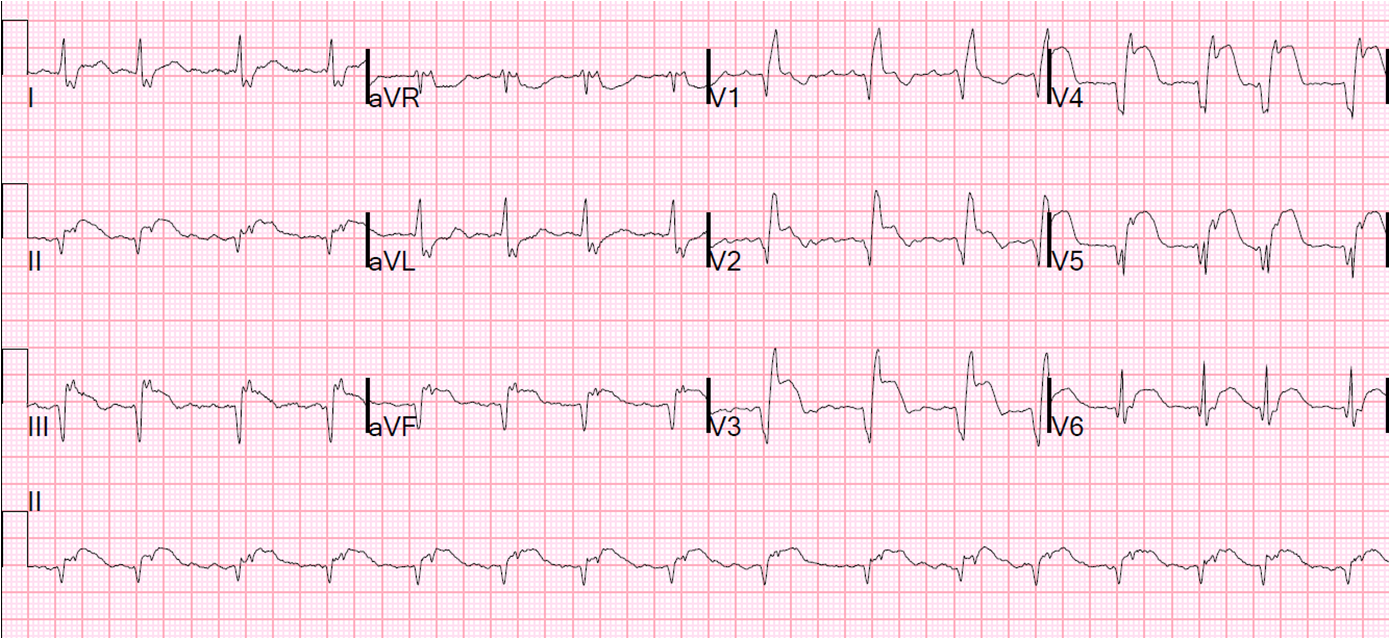
repaired Tetralogy of Fallot presented with CP. Here is her presenting ECG:
 |
| Sinus rhythm. Right bundle branch block (RBBB) and left anterior fascicular block (LAFB) with very high voltage, consistent with RV hypertrophy (RVH) due to Tetralogy (remember there is a constricted outflow tract of the pulmonary artery, leading to RV hypertrophy.) There is no initial r-wave of the rSR’ – there are initial Q-waves. The expected ST depression in V2 and V3 is not there, and in fact there is ST elevation in V3, as well as V4-V6. There is also some ST elevation in I and aVL. This is all consistent with either acute or old MI with persistent ST elevation. |
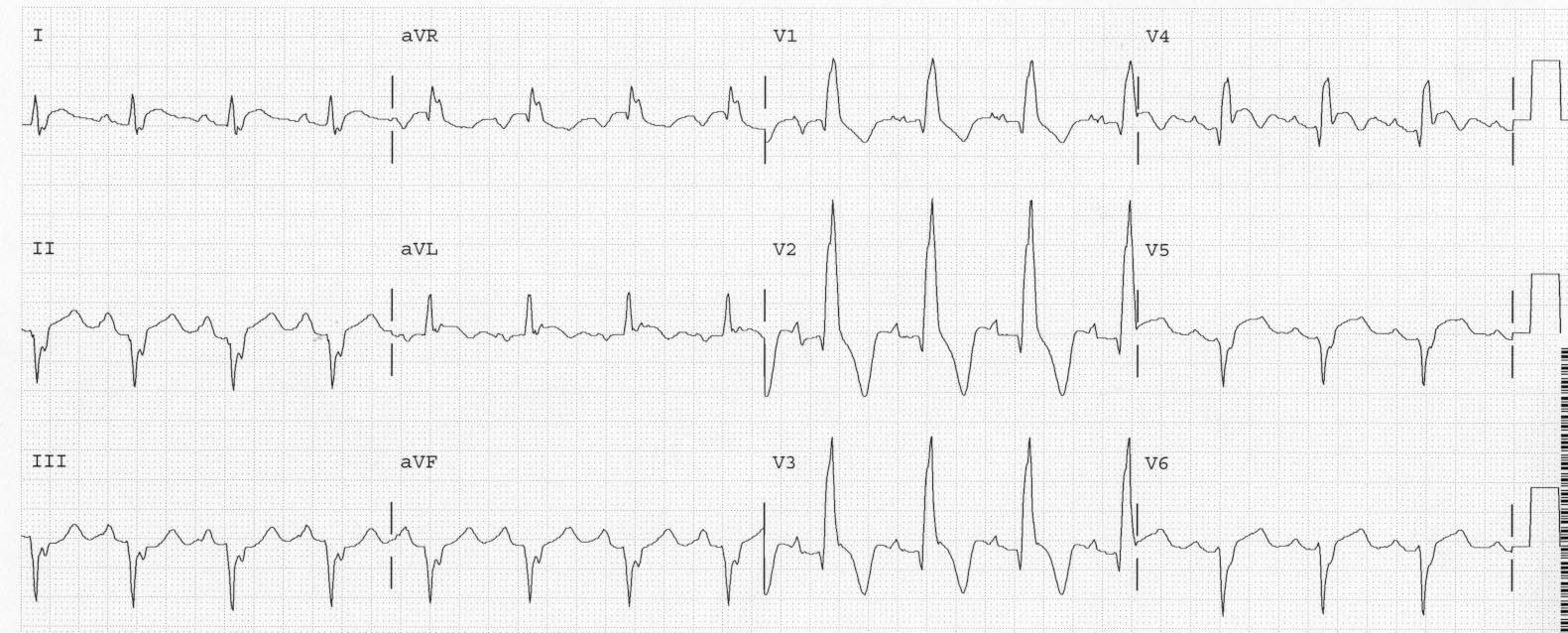
I was very suspicious of anterior STEMI, and found a previous ECG from 4 months prior:
 |
| Very large RR’ in V1: RBBB and RVH, also LAFB
Baseline ST depression in V1-V3, typical for RBBB. There is no ST elevation anywhere, also typical for RBBB. |
So there is relative ST elevation in V2 (relative to the previous ST depression) and new ST elevation elsewhere.
An
immediate echo confirmed new anterior-apical-septal wall motion
abnormality, as well as RVH and LVH, and the patient was taken for
angiography, which revealed fresh non-occlusive thrombus in the left
main that extended down and occluded the LAD. The patient went for
bypass surgery.
Lessons:
1. RBBB should not have ST elevation at baseline
2. In RBBB, there should be some ST depression in V2 and V3. An isoelectric ST segment may represent relative ST elevation.
3. A previous ECG can be very helpful
4. Echocardiography did confirm the findings, but delayed therapy. The ECG was diagnostic.
5. ST elevation can be found even when the QRS
appears very distorted.