Case written by Neha Ray MD, Brandon Fetterolf MD, and Pendell Meyers MD
A woman in her 40s with a history of rheumatoid arthritis, anemia, and thrombocytopenia presented to the ED with acute onset chest pain starting around 5am on the morning of presentation. It woke her from sleep. The chest pain was midsternal, severe, sharp, and constant.
On the previous night she had had a mild version of the same pain that she thought was heartburn (esophageal reflux). She reported some radiation to the left arm. She also reports 3 episodes of non-bloody vomiting over the course of the morning. She had a recent admission for endoscopy and colonoscopy which failed to show any source of bleeding. She denied any fevers, chills, sick contacts, diarrhea, or abdominal pain.
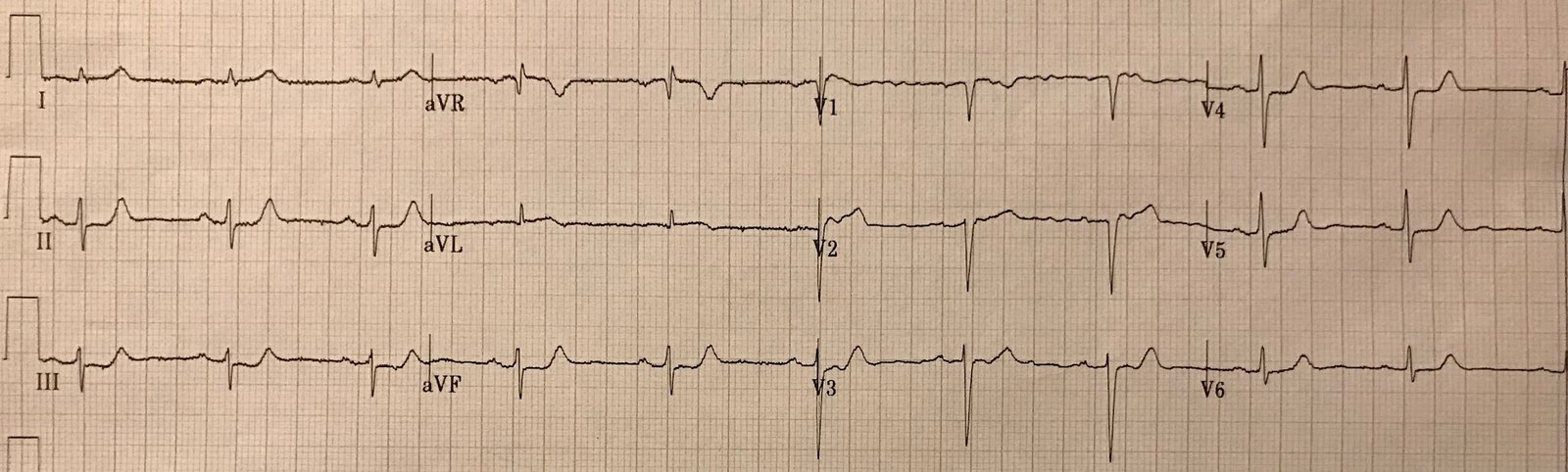
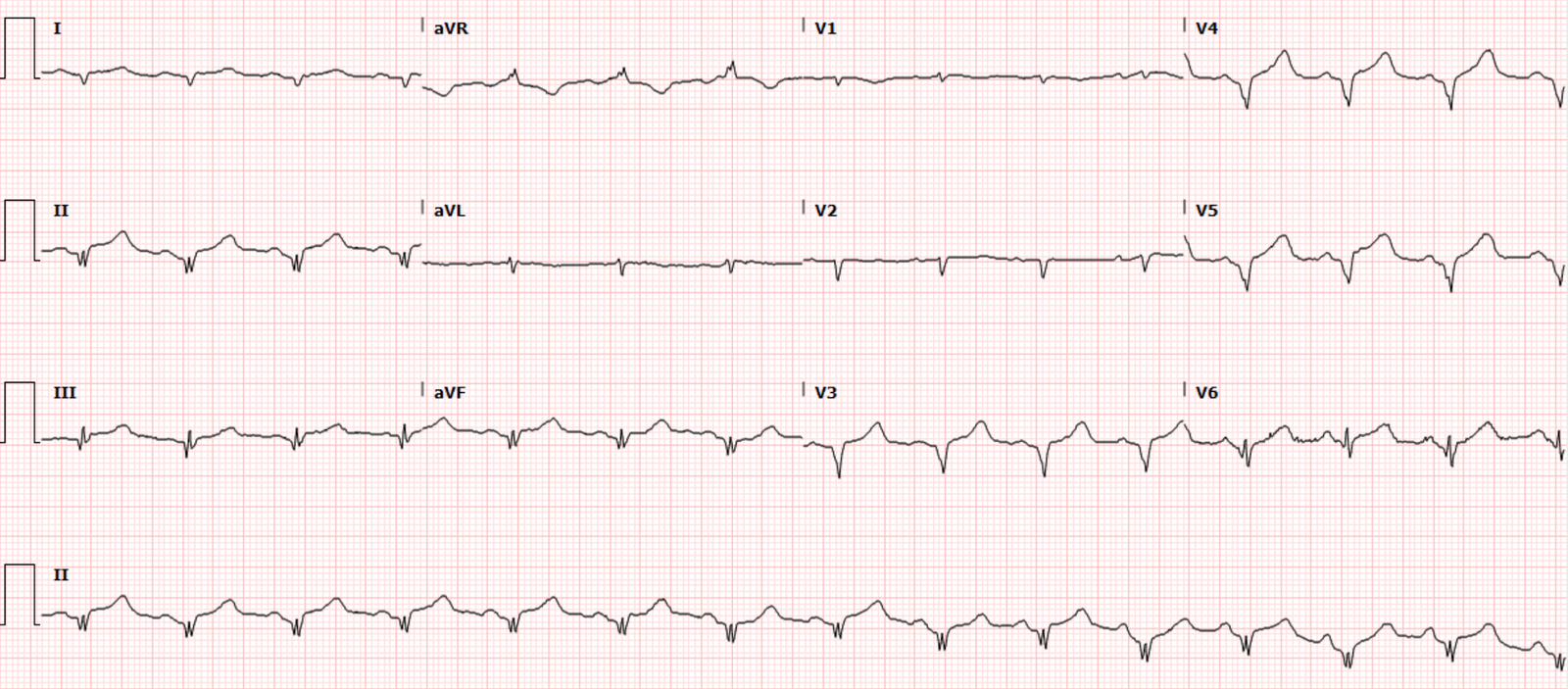
Here is her triage ECG:
 |
| What do you think? |
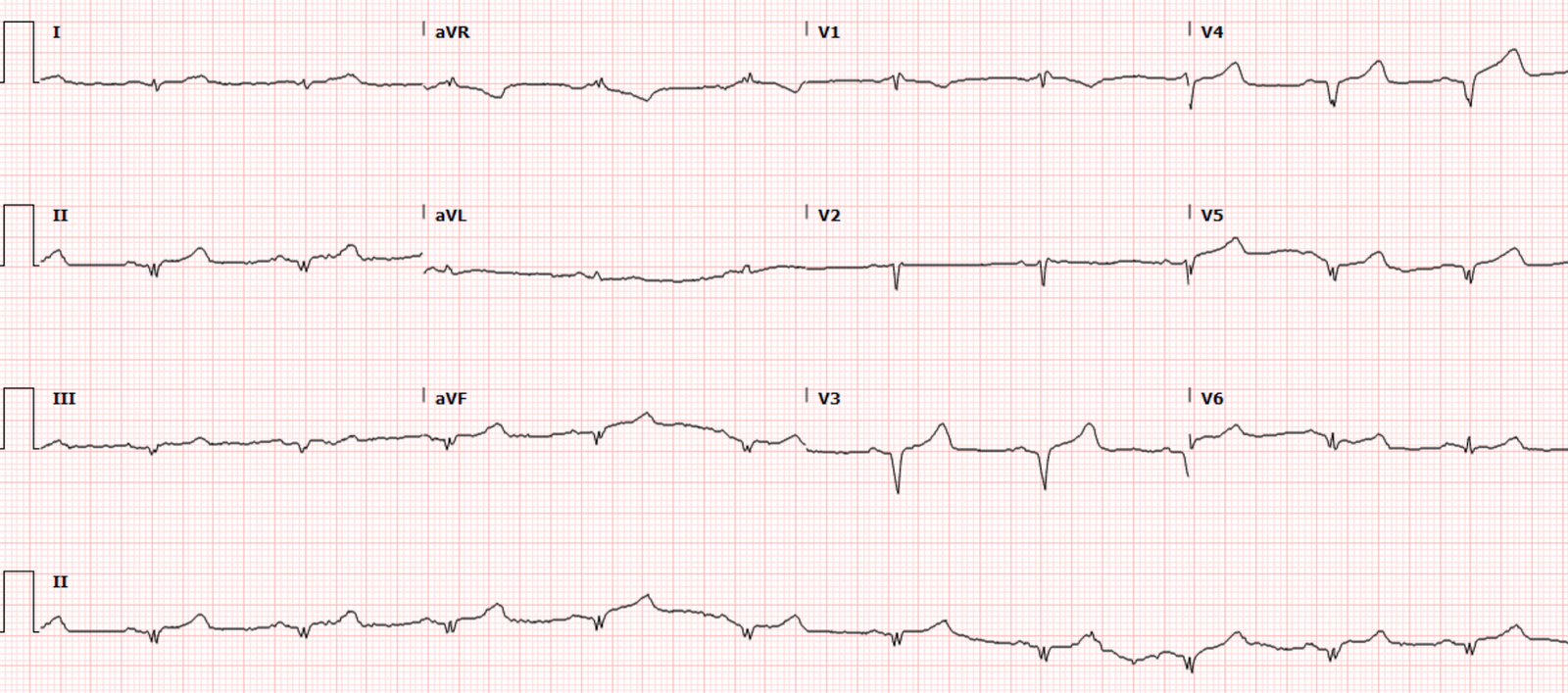
An old ECG from 4 years ago was available:
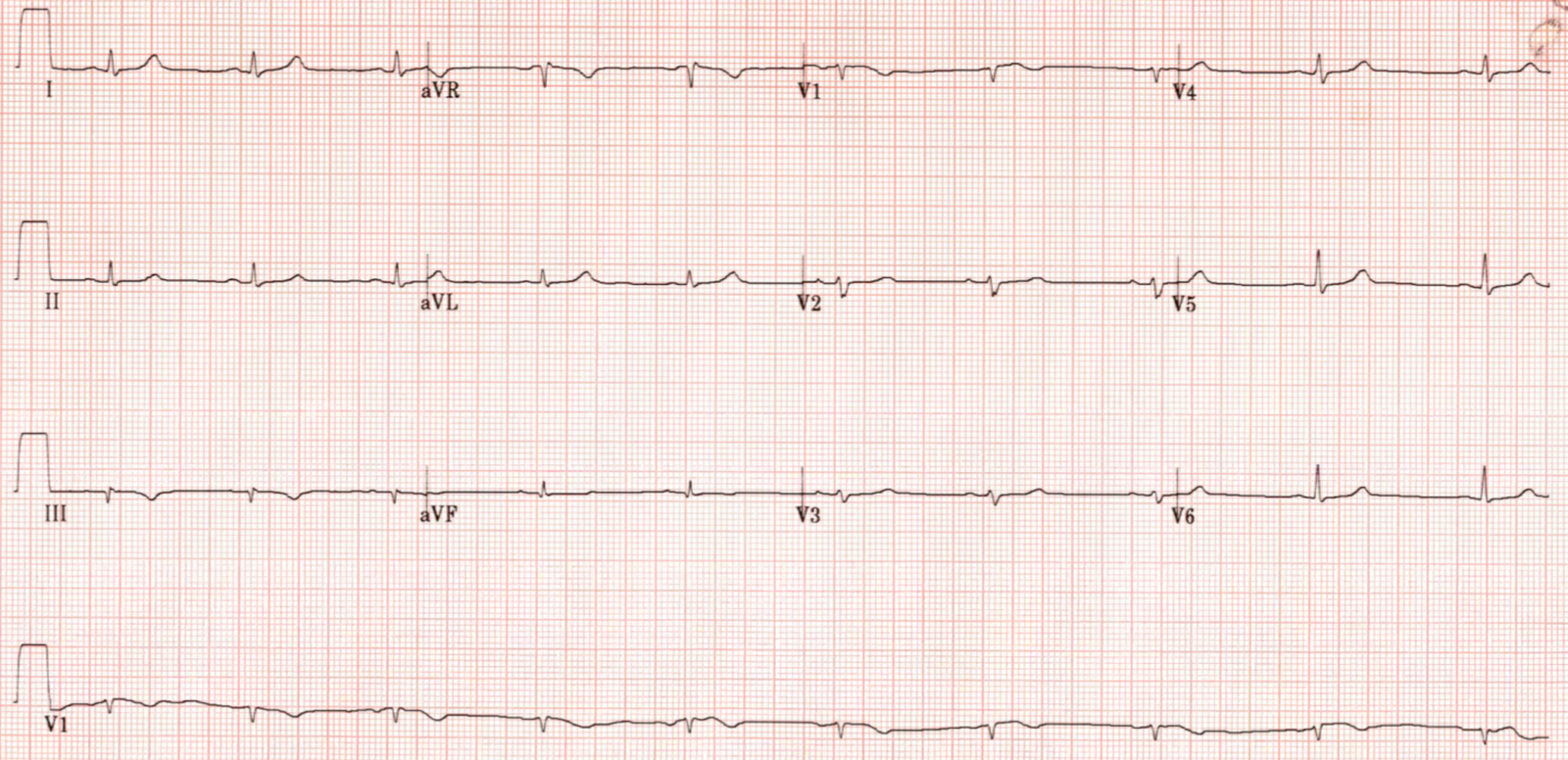
In the first rule, if there is any single T/QRS ratio in V1-V4 that is greater than 0.36, it is likely STEMI: for the ECG from 3 years prior, that would be lead V2. At 5mm/21mm, the ratio is less than 0.36 and would indicate LV aneurysm. But for the first acute ECG above, lead V2 is 8.5/15 which is 0.56 and would NOT indicate LV aneurysm.
In the second rule, one takes the sum of T-wave amplitudes in V1-V4 and divides by the sum of the QRS amplitude in V1-V4. A value less than 22 indicates LV aneurysm. In the second ECG from 3 years ago, that comes to 10/47 = 0.215, consistent with LVA.
T/QRS ratio to differentiate anterior STEMI from anterior LV aneurysm:
Validation (Klein, Shroff, Smith): Electrocardiographic criteria to differentiate acute anterior ST-elevation myocardial infarction from left ventricular aneurysm
https://www.ajemjournal.com/article/S0735-6757(15)00190-4/fulltext
Derivation (Smith): T/QRS ratio best distinguishes ventricular aneurysm from anterior myocardial infarction
https://www.ajemjournal.com/article/S0735-6757(05)00081-1/fulltext
ED bedside limited cardiac echo (performed by Drs. Dominic Nicacio and Gabriela Rivera-Camacho):
The parasternal long axis view above appears to show hypokinesis of the anterior septum.
The parasternal short axis view above appears to show hypokinesis of anterior septum and anterior wall.
With the ECG as it is, there will always be a wall motion abnormality. The question is: is it new or old? It can be very difficult to tell on bedside echo. If it is old (i.e. aneurysm) a very high quality echo might see wall thinning and diastolic distortion. If it is new, there will be a thick wall and no distortion. But usually bedside echo would not be able to make this distinction.
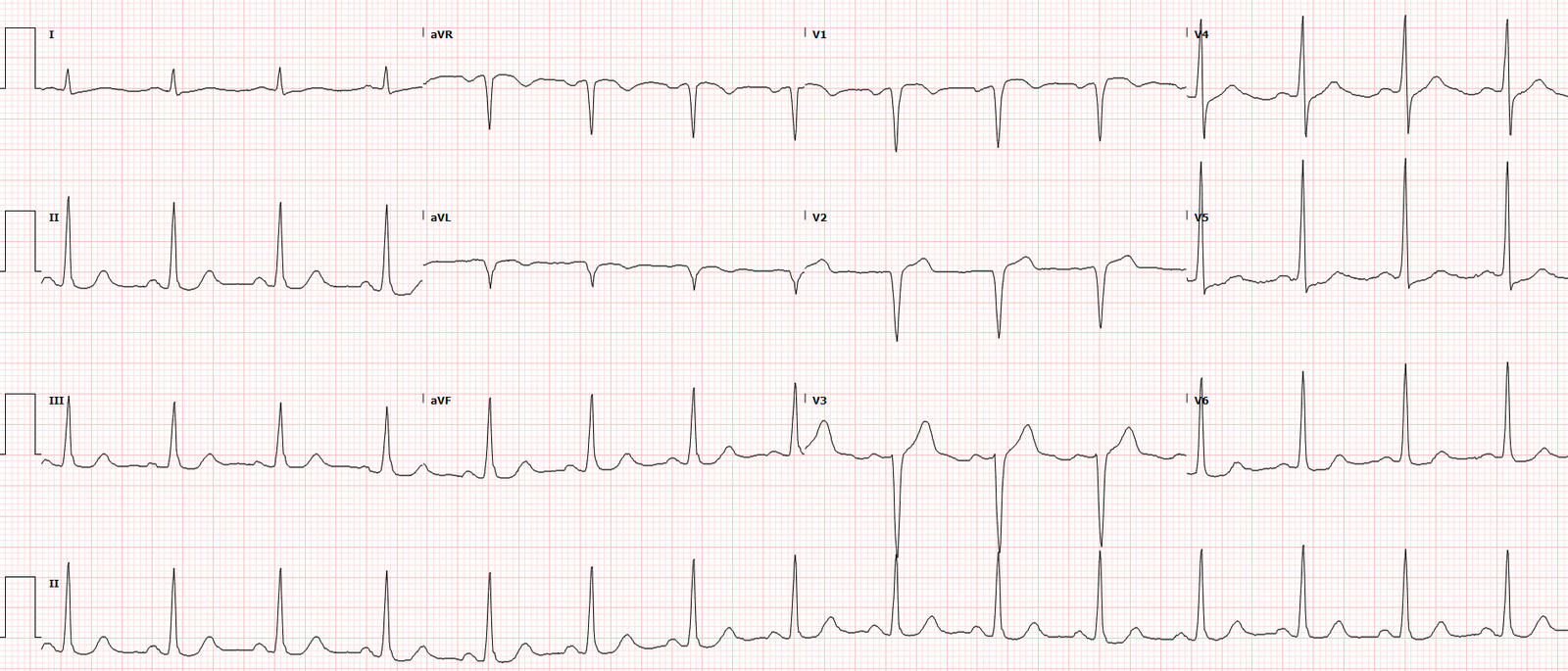
Repeat ECG about 1.5hrs later:
The repeat ECG shows worsening STE and persistent hyperacute T waves. The QRS complexes especially in the inferior leads are proportionally tiny compared to the ST segments and T waves.
The initial troponin (high sensitivity troponin I) returned highly elevated at 5,478 ng/L. This is consistent with the Q-waves on the ECG, and together they confirm some irreversible myocardial necrosis. However, this in no way means that there is no remaining salvagable myocardium if the patient undergoes emergent reperfusion therapy.
The patient was taken for emergent cath which showed a fully occlusive spontaneous coronary artery dissection of the proximal LAD. There was also an acute spontaneous nonocclusive dissection of the distal RCA. There was no aortic dissection. The occlusive LAD dissection underwent PCI with 3 overlapping stents. The nonocclusive RCA dissection was treated conservatively without PCI.
The next four serial troponin measurements were all greater than 25,000 ng/L (the assay does not report higher concentrations).
Her formal echocardiogram showed an EF of 25-30% with akinesis of the anteroseptal, apical, anterior, and lateral myocardium.
Her medical regimen was complicated by platelets of 2,000/uL (history of chronic low platelets). Hematology was consulted and the patient was transfused platelets with a goal of greater than 5,000/uL, at the same time he was continued on ticagrelor (the reasoning being that ticagrelor may have favorable pharmacokinetics in the setting of platelet transfusion). Aspirin was considered contraindicated.
Repeat echocardiogram on day 3 showed improvement of the EF to 43%, but still with severe hypokinesis in the same location.
She remained on ticagrelor monotherapy and had no bleeding issues. She was discharged home but long term follow-up is unavailable.
See these related cases:
Subtle Anterior STEMI Superimposed on Anterior LV Aneurysm Morphology
ST Elevation: is it due to old MI (LV aneurysm) or to acute STEMI?
ST Elevation and QS-waves in a patient with Dyspnea
Tachycardia and ST Elevation.
This ECG is nearly pathognomonic. What is it?
Subtle Anterior STEMI Superimposed on Anterior LV Aneurysm Morphology
Is this acute STEMI? LV Aneurysm? Would you give Thrombolytics?
ST elevation and QS-waves. ECG is equivocal. Use ED Echo!!
Hyperacute T waves examples:
10 Cases of Inferior Hyperacute T-waves
Ten (10) Examples of Hyperacute T-waves in Lead V2 (a few in V3), due to acute LAD occlusion
Ten cases of hyperacute T-waves in V4-V6
http://www.emdocs.net/hyperacute-t-waves/
https://www.emra.org/emresident/article/stemi-equivalents/