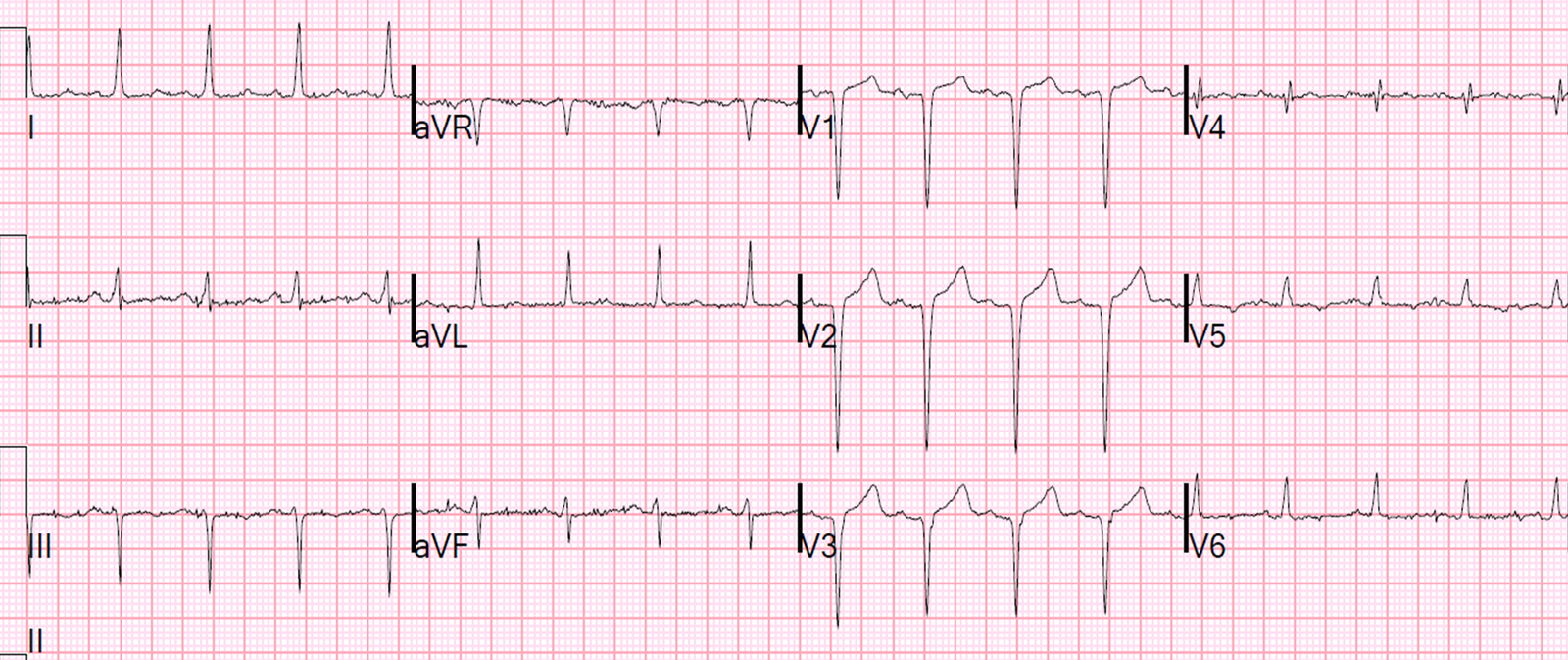
A middle aged male was resuscitated from cardiac arrest (ventricular fibrillation). Here is his initial ECG. He was hypotensive.
 |
| Besides the Atrial Fibrillation, what do you think? |
There is a slightly wide QRS, at 115 ms (by the computer). It is not quite a bundle branch block, but rather a nonspecific intraventricular conduction delay (IVCD). There are QS-waves in V3 and V4, and a QR-wave in V6. There is some minimal ST elevation in V4 and V5, but in V4 it is not excessively discordant (if we can apply modified Sgarbossa rules even in nonspecific intraventricular conduction delay) and in V5 it is not concordant to the majority of the QRS, nor is it excessively discordant.
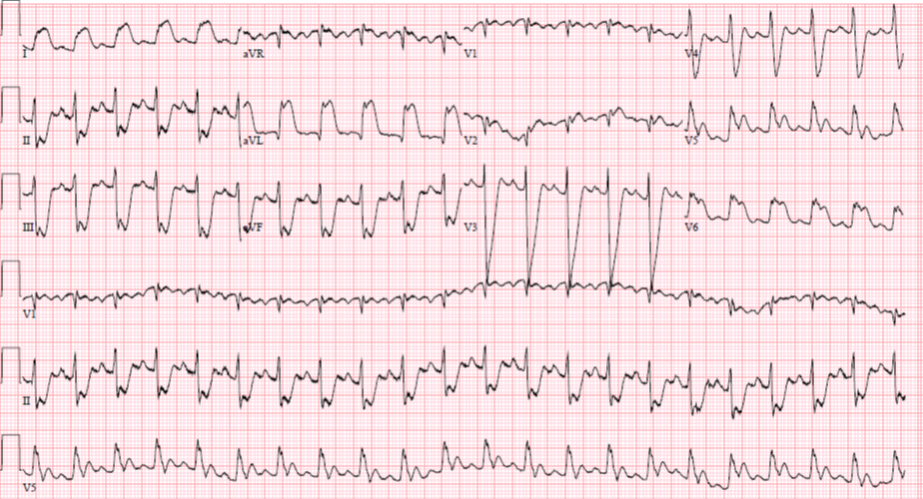
He underwent synchronized cardioversion into sinus rhythm, after which his blood pressure normalized. Then had the following ECG recorded:
 |
| What do you think? |
Analysis
The QRS is 116 ms. It looks like IVCD with left ventricular aneurysm morphology. Is it:
1. Simply persistent ST elevation after old MI (LV aneurysm morphology)?
2. Acute STEMI?
3. Subacute STEMI?
4. LV aneurysm with acute STEMI superimposed?
This is not at all an academic question: Both LV aneurysm and acute STEMI can cause VF arrest.
Hint: The ST elevation in V4 and V5, and the T-wave amplitude, appear to be too great for simple persistent ST elevation.
Is there a way to differentiate anterior LV aneurysm morphology from acute anterior STEMI?
Yes. We have derived and validated (abstract in press) two similar formulas with moderate accuracy (85-87%), with sensitivity for acute STEM of about 90% and specificity of about 70%. We also showed that they are more specific than another rule that uses QRS fragmentation. The two formulas rely on the fact that acute STEMI not only has ST elevation, but has a prominent T-wave.
Rule 1: if there is any T-wave to QRS amplitude ratio among leads V1-V4 that is greater than 0.36, then it is likely to be acute STEMI.
Rule 2: if the sum of T-wave amplitudes in V1-V4 divided by the sum of QRS amplitudes in V1-V4 is greater than 0.22, then it is likely to be STEMI, not LVA
Outcome
The patient was cooled and taken to the cath lab. There, a long acute mid-LAD 95% lesion with thrombus and low flow was seen and opened and stented. There was also complex 3-vessel disease but the acute lesion was in the LAD.
Subsequently, records from another hospital revealed that he had a history of ischemic cardiomyopathy and of LV aneurysm with LV thrombus. The thrombus had since resolved.
Here is the post-cath ECG:
 |
| The T-wave amplitude is diminished, and the ST elevation is also diminished. |
Now apply the rules:
Rule 1: V2 has 16.5/18.5 = 0.35, which is less than 0.36
Rule 2: (1.5 + 6.5 + 4 + 1) divided by (14.5 + 21.5 + 20.5 + 5 = 13/61.5 = 0.21 which is less than 0.22
The ECG thus supports the diagnosis of LV aneurysm now that the acute STEMI is resolved.
Formal echocardiogram confirmed dyskinesis (aneurysm) of the distal septum and apex. EF was 16%. Peak troponin I was 22 ng/mL.
Diagnosis:
LV aneurysm with superimposed acute STEMI.