One of my residents who just graduated saw this patient and sent the case:
This 80-something patient presented with chest pain. He had recently had a pacer placed for complete heart block and had not had an angiogram at that time. Ischemia had not been suspected.
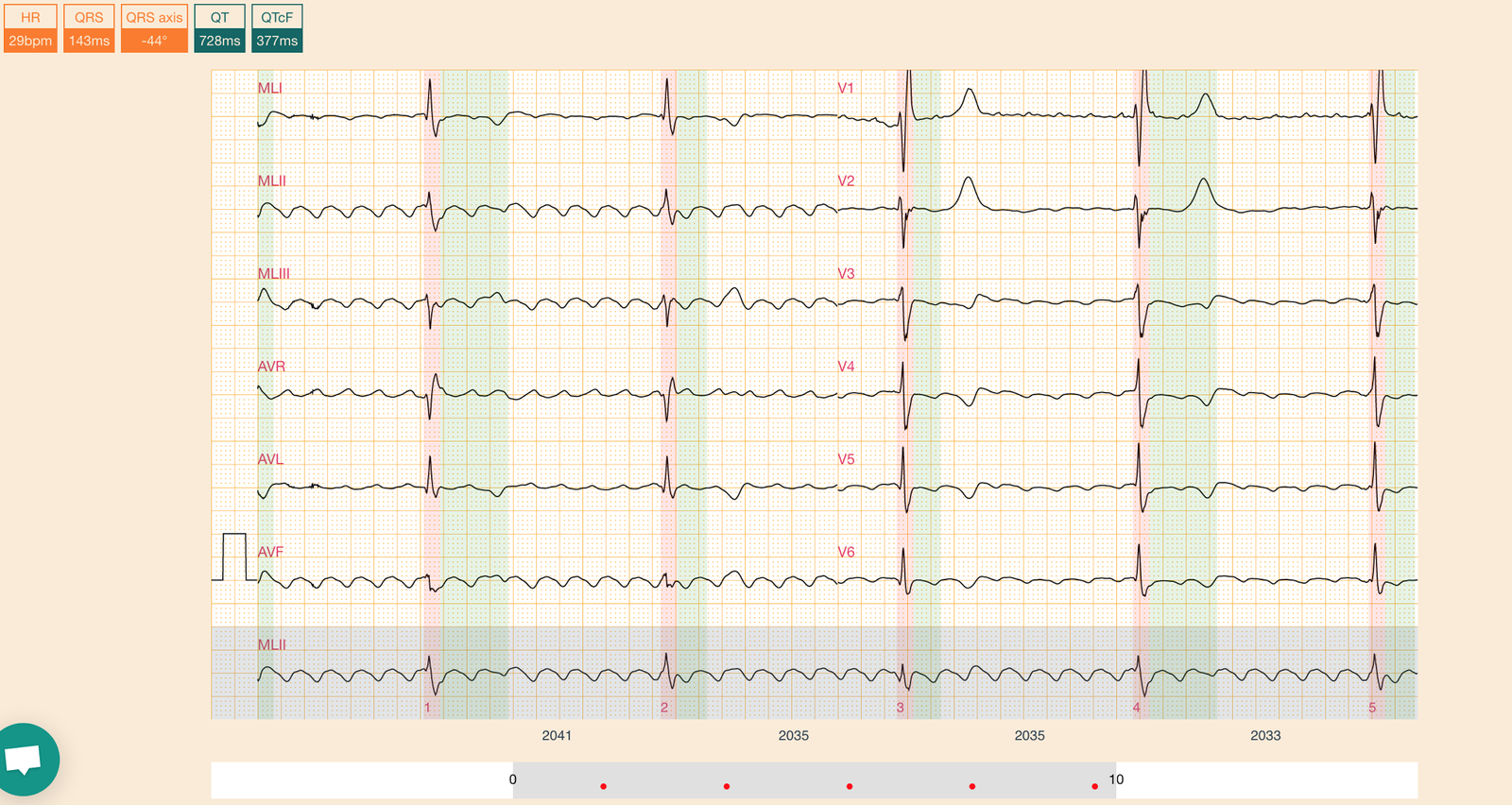
He had this ECG recorded:
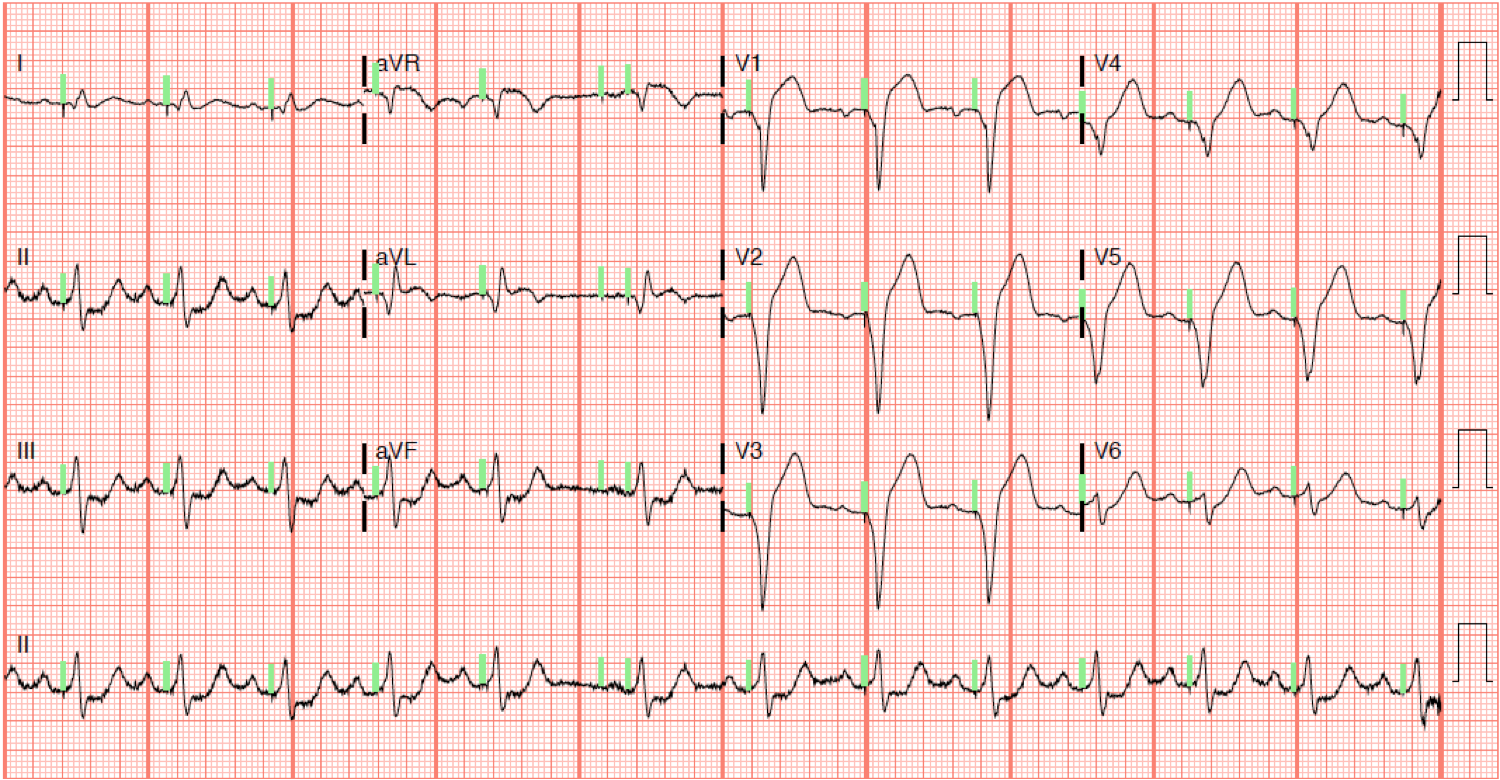 |
| There is sinus rhythm. There is clearly a DDD pacer that detects the sinus activity and then paces the ventricle (necessary when there is complete AV block). The pacing is in the right ventricle (all QRS negative in V1-V6, showing that the lead is in the apex of the RV).
Repolarization: There is reciprocal ST depression in II, III, aVF. There is discordant ST elevation [opposite to a negative QRS (i.e. S-wave)] in V1-V5. The cardiologist interpretation was “concerning for ischemia.” The ratio is 28% |
We do not know for certain what excessive is in paced rhythm.
The Smith-modified Sgarbossa criteria were derived and validated in Left Bundle Branch Block, which is similar to, but not the same as, ventricular paced rhythm. For LBBB, an ST/S ratio greater than 25% is very specific and sensitive for acute coronary occlusion.
Can we apply the rule to paced rhythm?
I don’t know for sure, but I do it and we are in the middle of a large multi-center study to try to figure it out.
Here it is: Paced Electrocardiogram Requiring Fast Emergent Coronary Therapy (PERFECT) Study. https://clinicaltrials.gov/ct2/show/NCT02765477
Importantly, 50% of physicians who care for patients with chest pain believe that you cannot diagnose STEMI in the presence of paced rhythm. This is definitely not true and an old teaching that should be thrown away.
The emergency physician activated the cath lab. He writes that “Cardiologist thought you could not see the ischemic changes on paced ECG.”
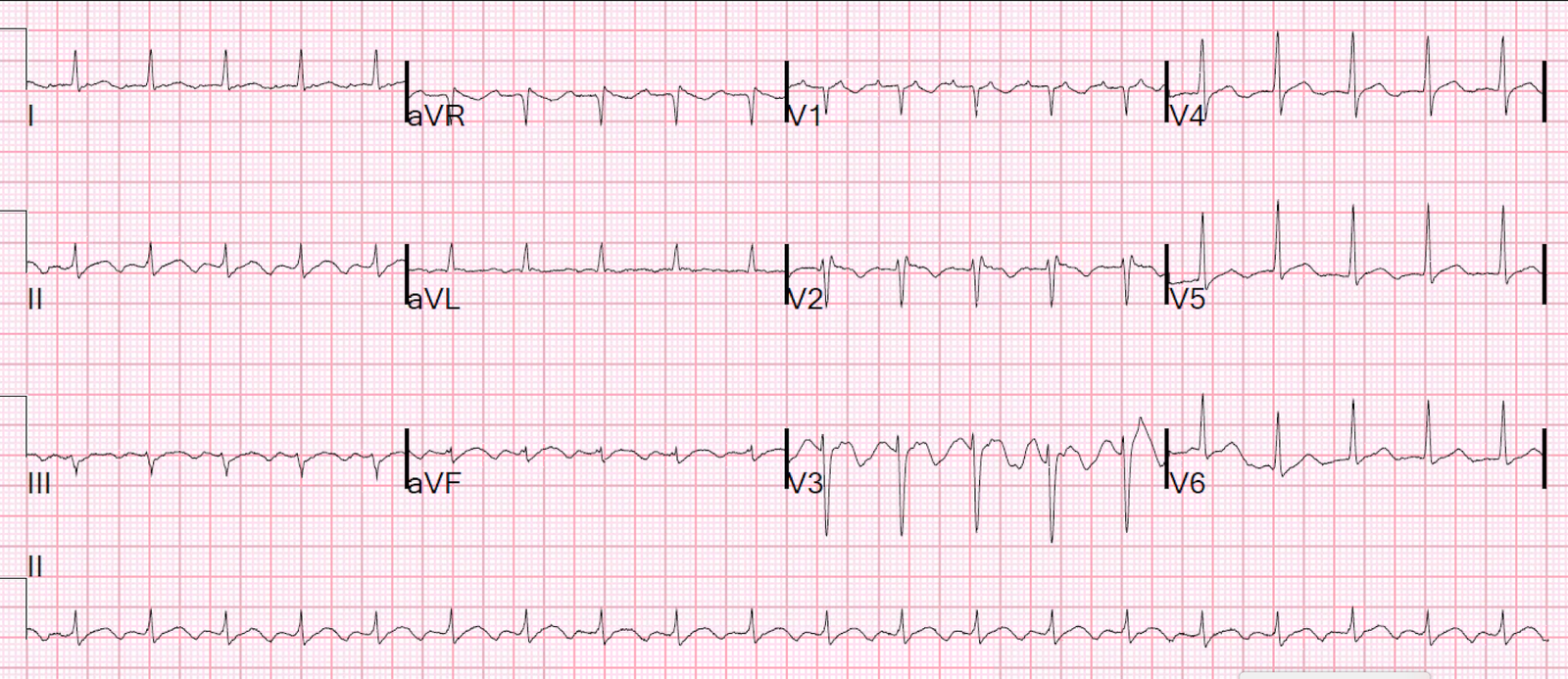
In the meantime, an old ECG was found:
 |
| The change is obvious and makes the first ECG diagnostic. The discordant ST elevation in V1-V3 in this old ECG is proportional. |
The patient had an acute 100% LAD occlusion.