Many believe that left main occlusion results in diffuse ST depression with ST elevation in aVR. This is not true, as I write about in this post: The difference between left main occlusion and left main insufficiency.
A 38 year old male presented with 6 hours of chest pain, and recent chest pain with exertion. He had no significant past medical history and was on no medications. He is a non-smoker. The initial troponin was 1.62 ng/mL.
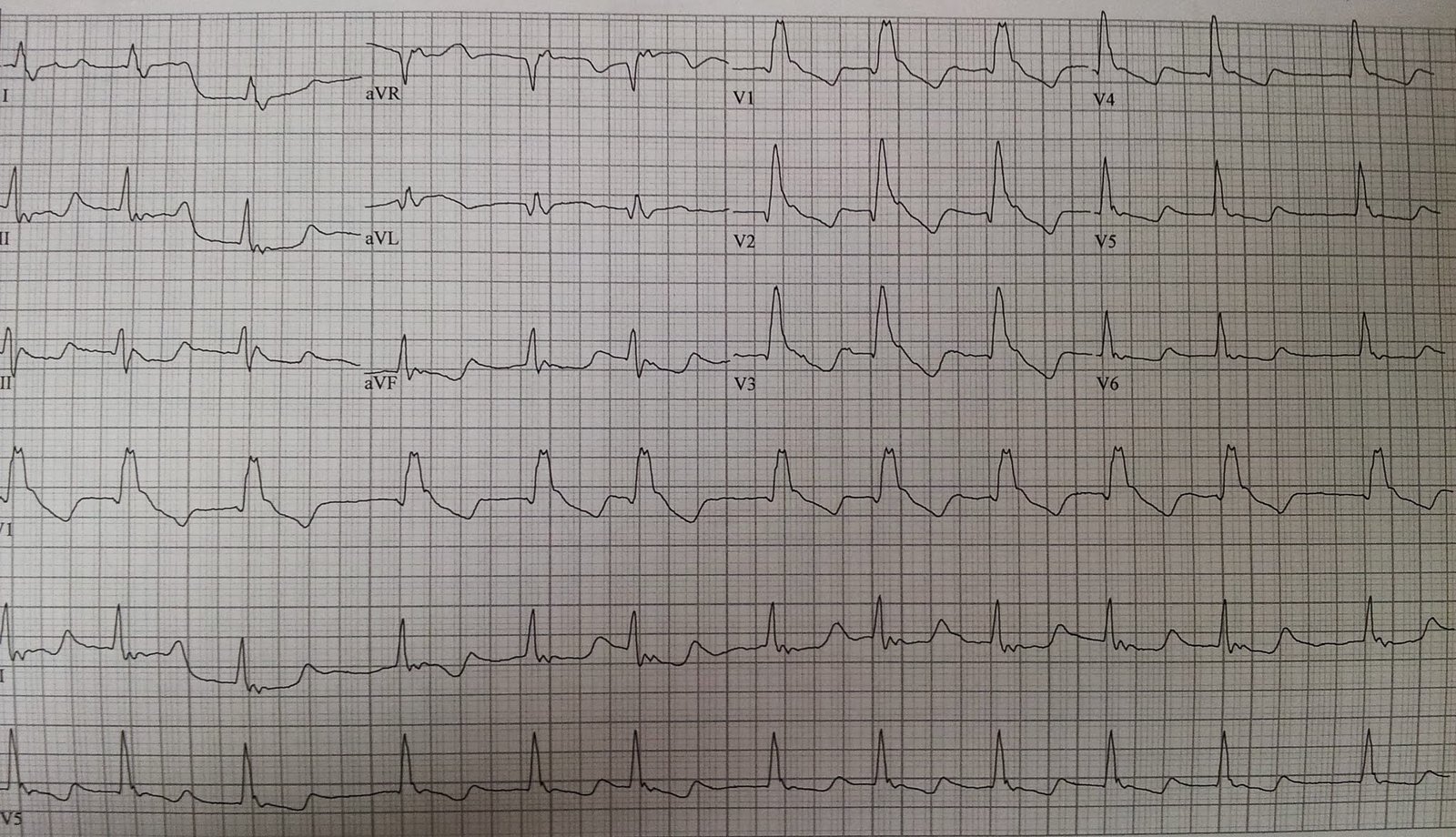
Here is the initial ECG:
 |
| There is diffuse ST depression, with ST elevation in aVR. This is consistent with coronary insufficiency, but not coronary occlusion. It could be a tight left main, or a tight LAD, especially with 3-vessel disease. There is ST elevation in lead III, with an ST axis directly to the left. Is there inferior STEMI also? |
Such patients have about a 50% chance of needing CABG, as shown in an article referenced and described in this post. Therefore, Plavix (clopidogrel) should be avoided.
The patient was taken for emergent angiogram:
 |
| This is an angiogram of the left main, and it is totally occluded. |
How is that possible? Why is the patient alive? And why is there ST depression of subendocardial ischemia rather than ST elevation of anterior, lateral, and posterior walls?
Why is this not a STEMI?
The answer lies in the RCA angiogram:
 |
| The distal RCA is seen on the left side of the image (we do not see the catheter or the injection at the ostium of the RCA. There are right to left collaterals which supply the left system with enough flow to keep the patient alive and to prevent subepicardial ischemia (STEMI). All of the flow seen on the right side of the image is flow in the LAD and circumflex that is supplied by the RCA collaterals. The apparent inferior STEMI may be due to “Coronary Steal Syndrome”: Right to left flow is stealing blood supply from the inferior wall. |
The left main was opened and the patient did well.
Most left main occlusions to not make it to the ED alive.
See this previous post for an extensive discussion (same link as above).