This most recent post will help you understand this post here:
I was nordic skiing out in the wilds of the Upper Peninsula of Michigan when I received a call on my iPhone from some colleagues. They texted me the following ECGs, which I viewed in the shade of a pine tree on a glorious sunny snowy landscape. AT&T surprised me with their reach.
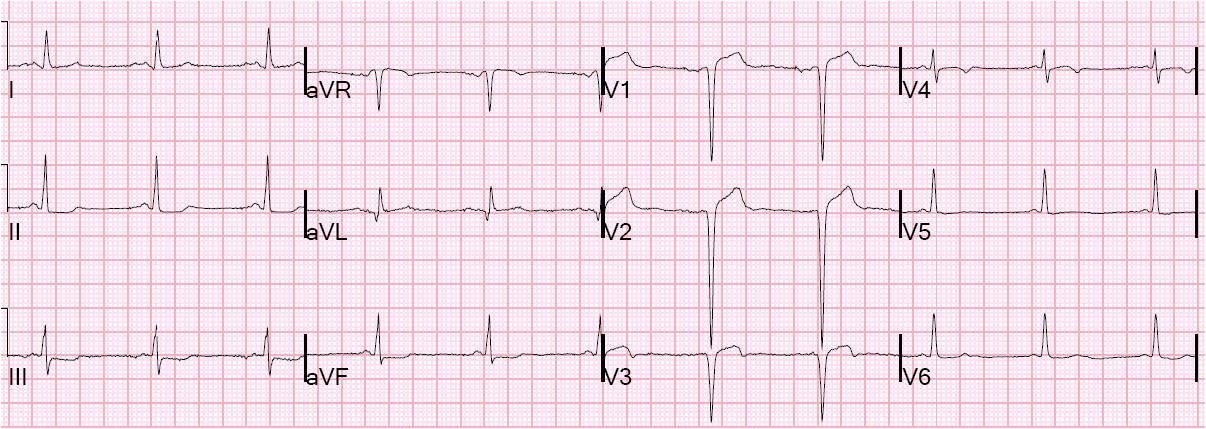
A 52 year old woman presented with chest pain. There was some pulmonary edema. This ECG was recorded at 1144:
 |
| There is ST Elevation in aVR and diffuse ST depression (I, II, aVF, V3-V6). Thus the ST elevation axis is towards the right, not posterior, not inferior. There is no ST elevation or depression in lead III, so the ST axis is perpendicular to III, towards aVR. This is typical for subendocardial ischemia, not STEMI, and often means left main ischemia or 3 vessel ischemia. |
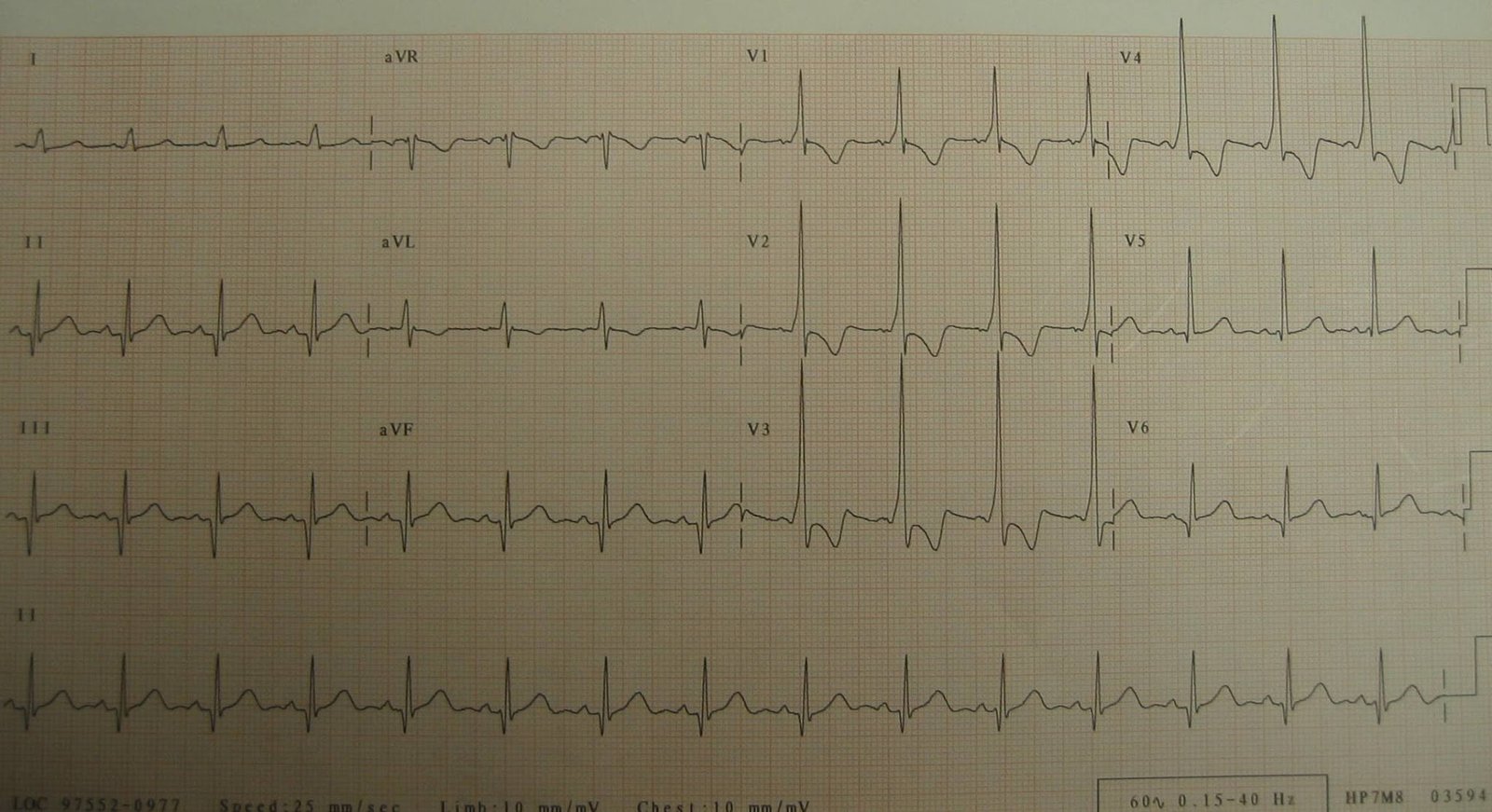
A right sided ECG was recorded 3 minutes later. Right sided ECGs are best recorded in the context of inferior STEMI. There is little utility to them in other situations, unless you suspect an isolated RV infarction. I’ll post one of those later.
 |
| There is quite a bit of ST elevation in V4R-V6R. Some is due to baseline wander, but not all. It looks like a right ventricular MI. There was no RVMI, though. This ST elevation is a reciprocal view of the left lateral ST depression. The ST vector is to the left and so this is what I would call a pseudo right ventricular MI. |
The physicians were very worried about RV MI. But STE in Right sided leads is to be expected when there is left sided ST depression and STE in aVR!!
Because of precordial ST depression, clinicians were also worried about posterior STEMI. But posterior STEMI is not likely when there is diffuse ST depression, with STE in aVR. It is likely when there is ST depression primarily in V1-V4. Posterior STEMI may also be accompanied by lateral STEMI, with ST depression in inferior leads (mostly lead III), but not in lead I.
Nevertheless, they recorded posterior leads [V4-V6 are moved to V7 (posterior axillary line), V8 (between V7 and V9), and V9 (paraspinal) (all are at the level of the tip of the scapula)].
 |
| There is no ST elevation in V7 “V4” to V9 “V6”. Positive would be 0.5 mm in just one lead. |
The patient was treated with NTG, aspirin, eptifibatide, heparin, and became pain free. Clopidogrel was avoided due to the high likelihood for need for bypass surgery, which can be complicated by the prolonged platelet inhibition of clopidogrel.
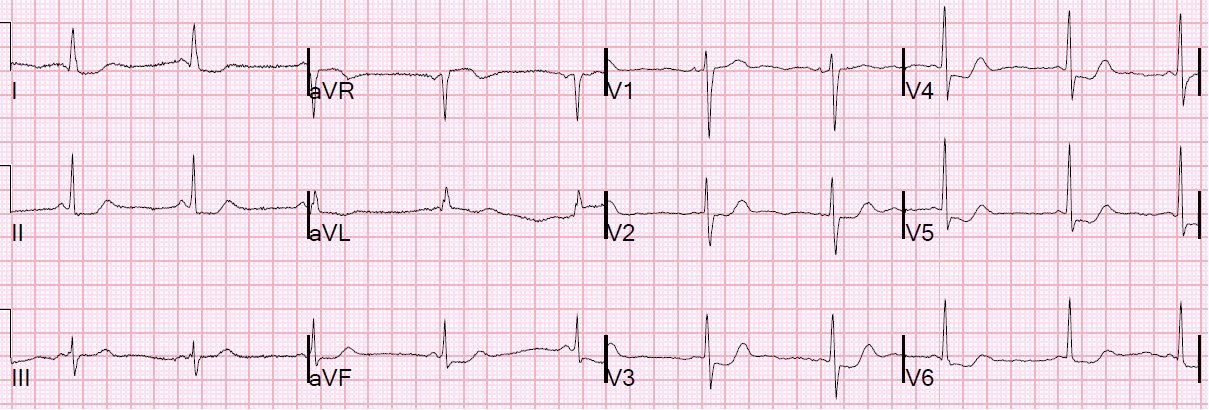
This is her ECG 1.5 hours later:
 |
| STE in aVR and diffuse ST depression are still present but less marked. |
Perusal of her charts revealed that she had an LAD stent that was very close to the ostium of the circumflex. Troponin I was positive and peaked at 4.88 ng/ml. Echo revealed inferior but mostly lateral hypokinesis. Cath the next day revealed that both the proximal LAD and the ostial circumflex had tight culprit lesions with intact flow. They were not amenable to PCI. She underwent successful CABG.
The RCA and the right ventricular branch were normal.