This is a 68 yo male with a history of aortic stenosis, on carvedilol, fell from a ladder approx 20 ft onto concrete, landing face down with likely loss of consciousness. Upon EMS arrival, pt was still face down in a pool of blood, but was responsive, alert, and neuro intact. His BP was stable en route, but he was bradycardic in the 30’s.
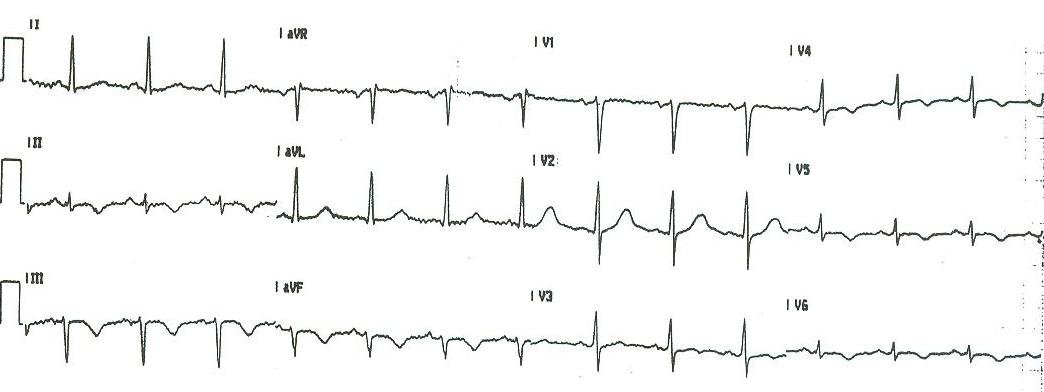
On exam, he had multiple orthopedic injuries, but no significant head, neck, spinal, chest, or abdominal injuries. The patient had had no premonitory chest pain or SOB. His BP was 121/59 and he was well perfused. This was his initial ECG:
 |
| There are regular p-waves at a rate of about 90, but they do not conduct. Thus, there is 3rd Degree AV block with a probable Purkinje escape at a rate of 36; the wide QRS and RBBB pattern (rSR’ in V1, wide S-waves in lateral leads) tell us that the escape is from the left bundle, creating an RBBB-like ECG. [Alternatively, there could be a nodal escape with RBBB]. There are also very wide, bizarre, inverted T-waves. The QT is 680 ms, and QTc = 527 ms. There are no ST changes indicative of STEMI. |
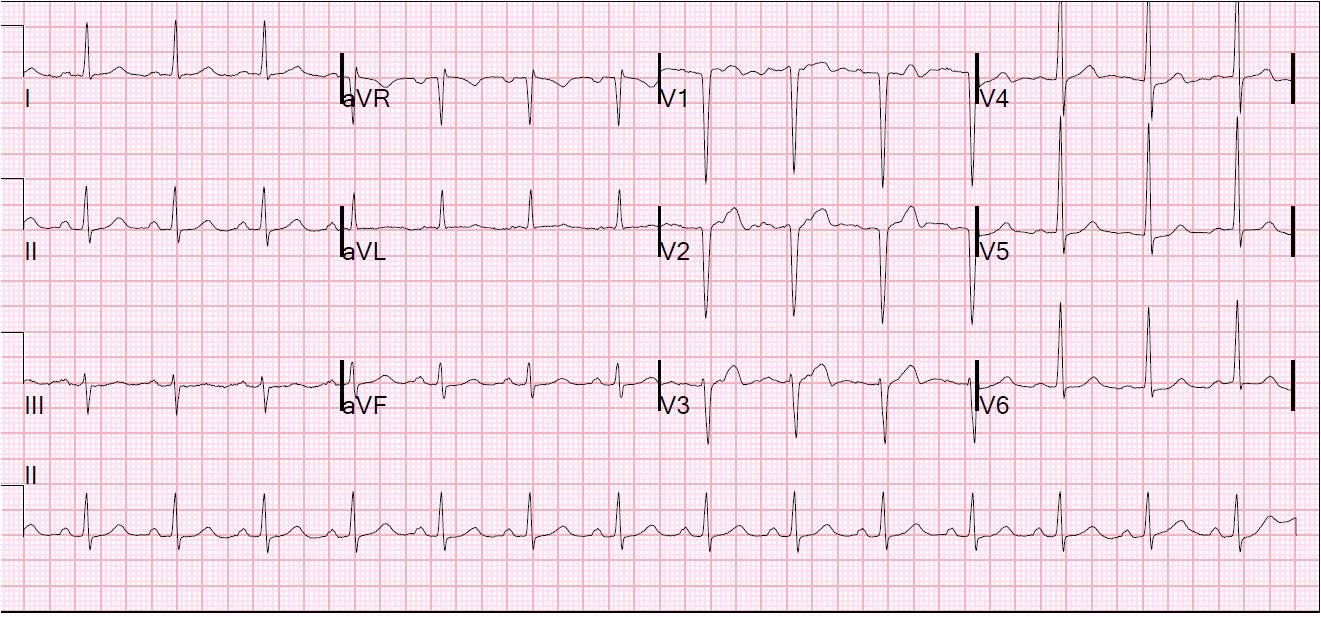
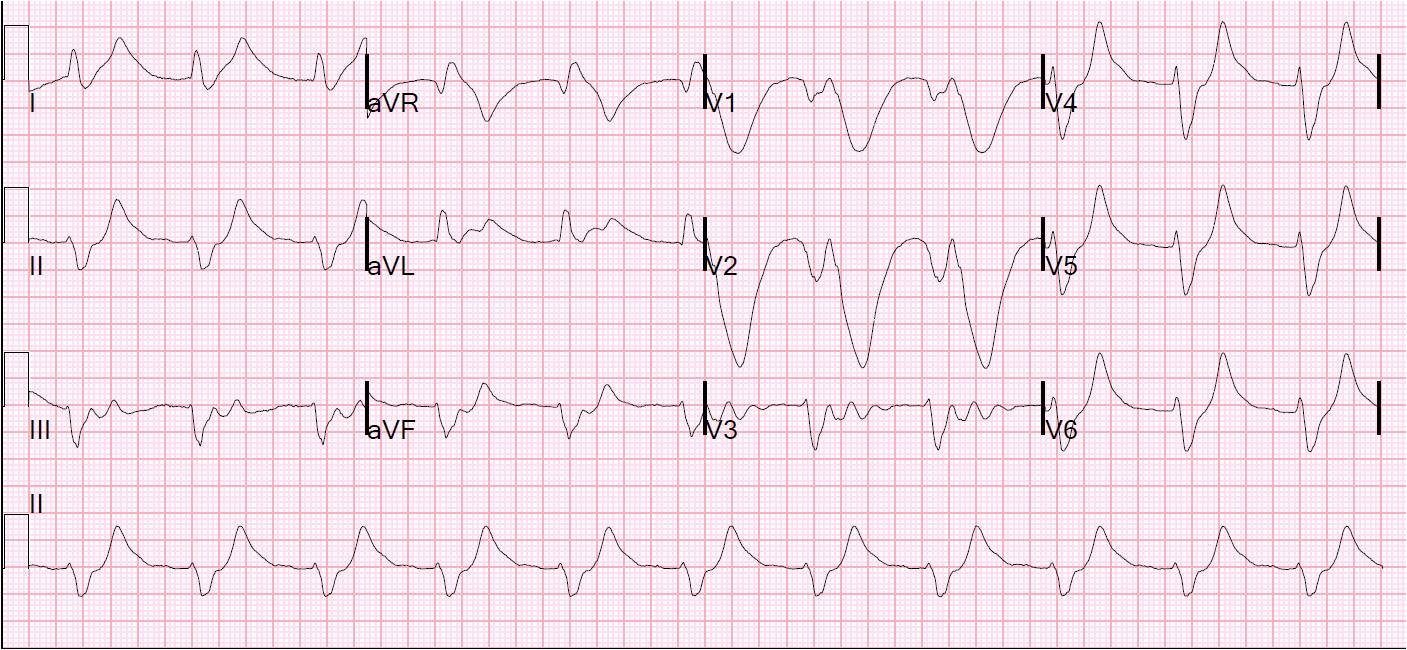
First troponin returned at 0.11 ng/ml (slightly elevated). With all his injuries, he spent 2 hours in the ED, and a subsequent ECG is shown here:
 |
| Now the escape has an RBBB in the first part of the ECG, and LBBB pattern in the latter part, and the rate is 41. The escape has alternated to the right bundle [or there is a nodal escape with LBBB]. |
This is a classic ECG. A drop attack with third degree AV block is called a “Stokes Adams” attack, and is often associated with bizarre wide inverted T-waves. A google scholar search comes up with several articles: Giant T-wave inversion associated with Stokes-Adams syncope (sycope due to complete AV block).
The escape rhythm is dependent on the automaticity of the tissue that escapes. AV nodal escape is the fastest, then HIS bundle, then Purkinje fibers, then ventricular tissue (which results in a slow “idioventricular” rhythm)
In this case, there is either an alternating escape, or a nodal escape with alternating RBBB and LBBB. If it is the former, then you know that your bundles have appropriate automaticity and can support the rhythm without a stimulus from above. If it is the latter, then you have the risk of developing block of both the left and right bundles simultaneously, in which case the only escape possible is idioventricular.
Obviously, this is a dangerous situation, and you must place transcutaneous pacing pads and ascertain that they will capture if you need them too. Alternatively, an internal pacing wire can be placed.
A simple test of capture is nicely done by pacing and observing the heart with bedside ultrasound to be certain of capture.
Case continued:
Fearing possible beta blocker toxicity, glucagon was given in increments up to a total dose of 5 mg, but this was not effective. Atropone 1 mg was given without effect (this will not work in this situation, ever). An internal pacing wire was placed in the ED, but not used because, in the interim, dopamine had been started and titrated to 10 mcg/kg/min with an increase in the heart rate to the 50’s. Pacer pads were also placed.
Subsequent troponins rose to a maximum of 8.5, suggesting that ACS may have had a role here. However, third degree heart block can develop for other reasons than acute MI.
An echocardiogram revealed moderately severe aortic stenosis with a valve area of 1cm2, with a mean pressure gradient of 50mmHg. There were regional wall motion abnormalities (apex, distal septum and
inferior) but these are difficult to interpret in the setting of LBBB.
Angiography and Ventrilography revealed worse AS, with valve area of 0.74 cm2. There was no coronary artery disease.
A permanent pacer was placed on hospital day 3.
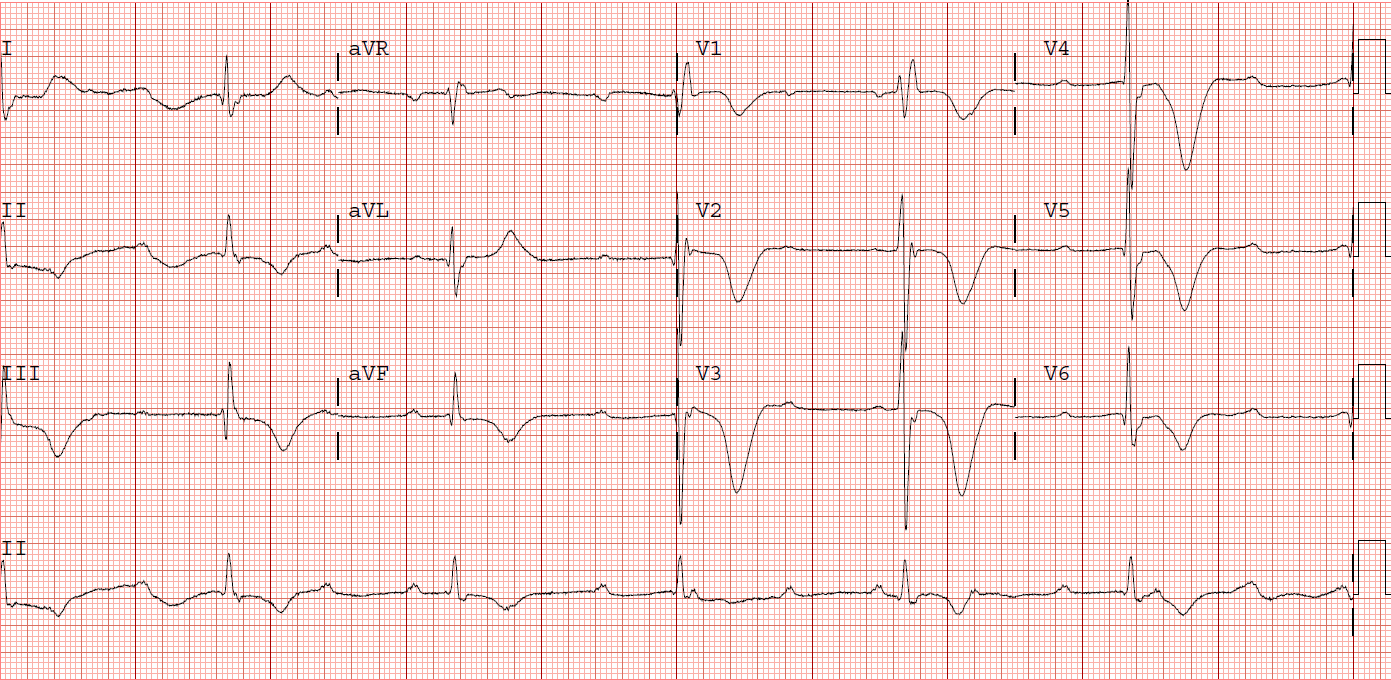
This is the final ECG:
 |
| Perfectly normal paced rhythm. Note that all precordial QRS are negative. This is because the pacing lead is placed in the apex of the right ventricle, so that depolarization always proceeds away from the apex of the heart (on the chest, the point of maximal impulse). Thus, it depolarizes away from all precordial leads. |
After many orthopedic procedures, the patient had his aortic valve replaced, and went home.