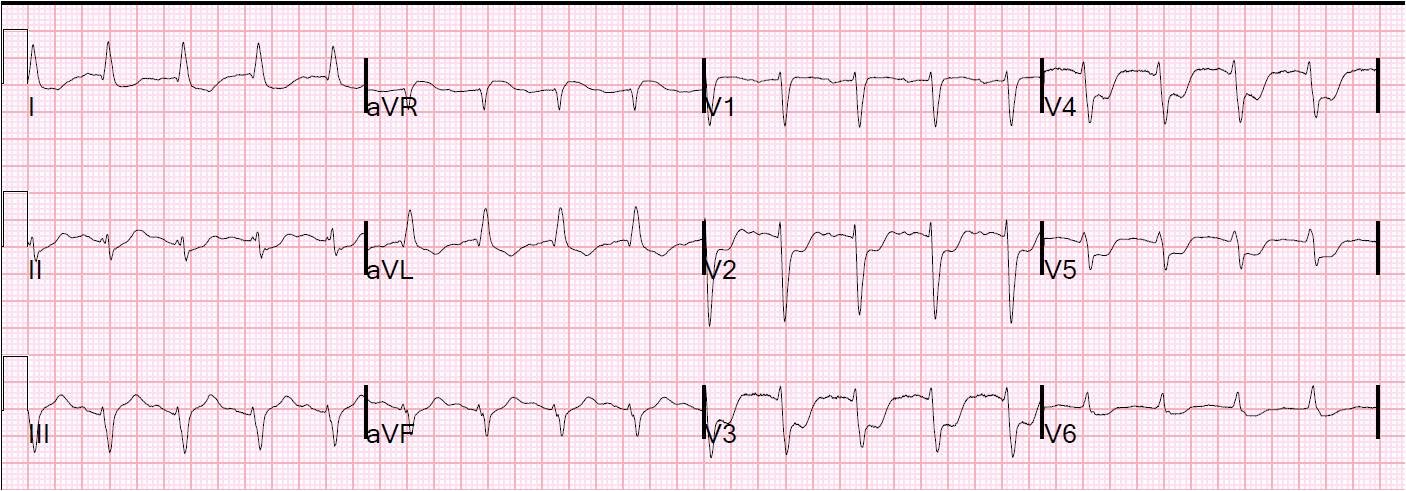
A 68 yo female with a history of HTN on metoprolol and of paroxysmal atrial fib presented with weakness. This is her ECG.
There is sinus bradycardia at a rate of about 55, with a p-wave every 1.05 seconds. There are 2 dropped p-waves. The succeeding p-wave in each case is exactly 2.1 seconds later. This means that the sinus node continues to depolarize and do its pacemaking job every 1.05 seconds, but that occasionally that signal fails to leave the sinus node and get to the atrium where it would depolarize the atrium resulting in a p-wave.
Notice that the p-wave that comes directly after the 8th QRS conducts, but the one that comes after the 4th QRS does not. This is Ashmann’s phenomenon: the refractory period of a beat is longer when the preceding R-R interval is longer. In this tracing, it is not obvious (you must measure it), but the R-R inverval between R-waves 3 and 4 is longer than the R-R between R-waves 7 and 8.
She was also found to be hypothyroid.
This is sino-atrial exit block. The sinus node fires but it does not escape. The combination of bradycardia (exacerbated by metoprolol), with paroxysmal atrial fib and sino-atrial block are typical of sick sinus syndrome. It will inevitably progress to the point where a pacemaker will be necessary.