Written by Magnus Nossen
An 80-year-old man with a history of hypertension and paroxysmal atrial fibrillation contacted EMS due to episodes of chest pain. He stated he had been experiencing recurring episodes of chest pain over the last couple of days, lasting from a few minutes to half an hour. On the day of presentation, the CP became more intense, prompting him to seek medical attention. When EMS arrived, the pain had improved, and after administration of ASA and NTG, he reported complete symptom relief.
The ECG below was recorded by EMS. What do you think?
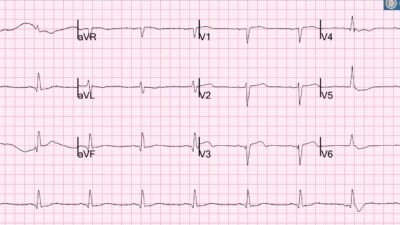
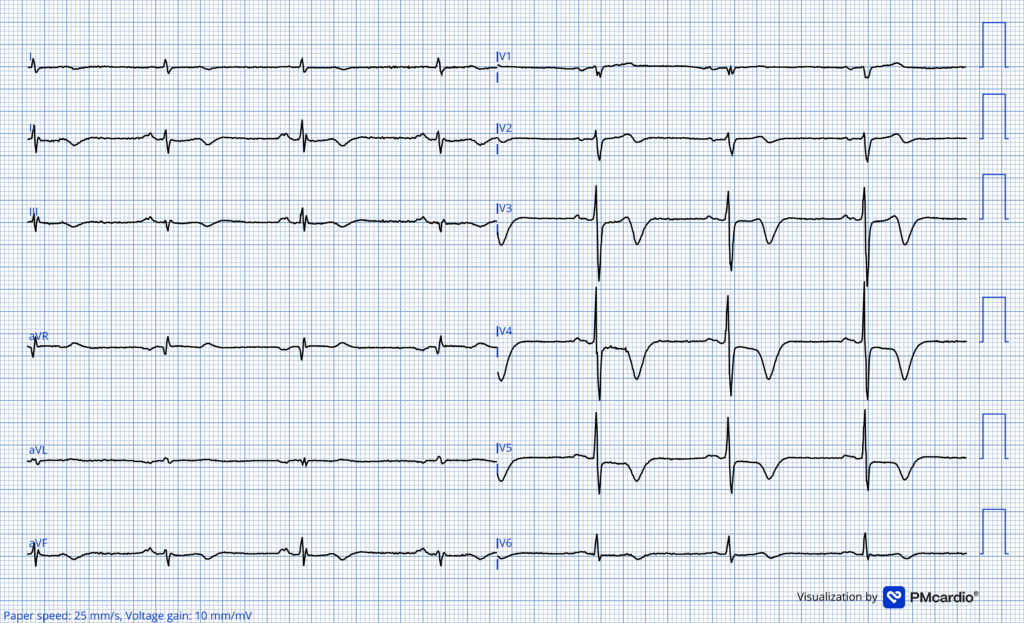
ECG #1 recorded by EMS
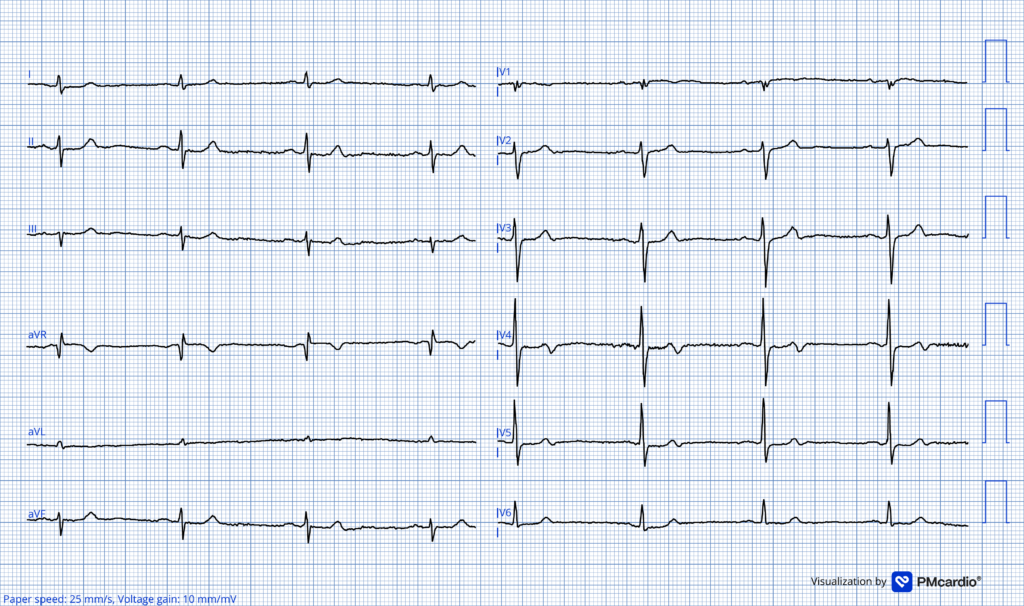
There is sinus bradycardia at 50 bpm. QRS complexes are narrow. There is no ST-segment elevation. There are terminal T wave inversions in leads V3–V5. These slight TWI in the setting of resolved chest pain, is most consistent with early post-ischemic reperfusion changes.
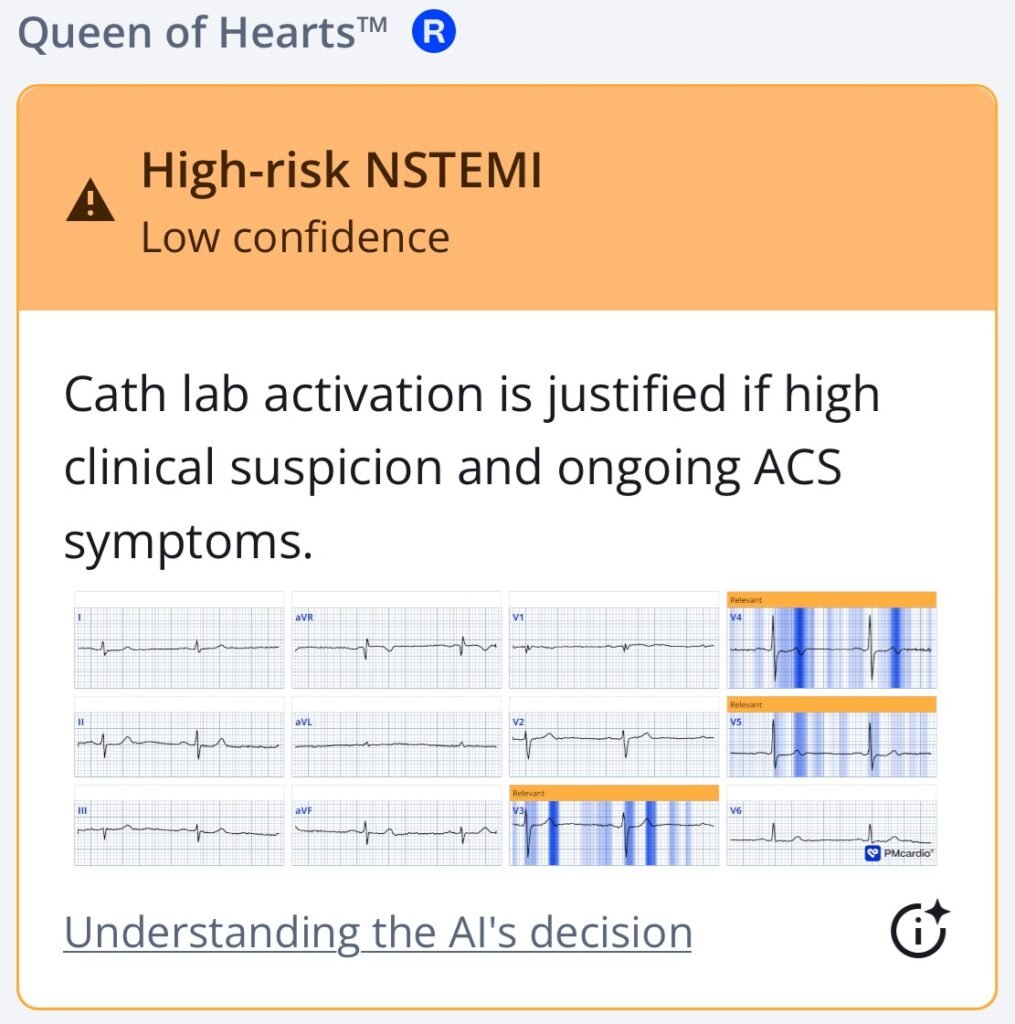
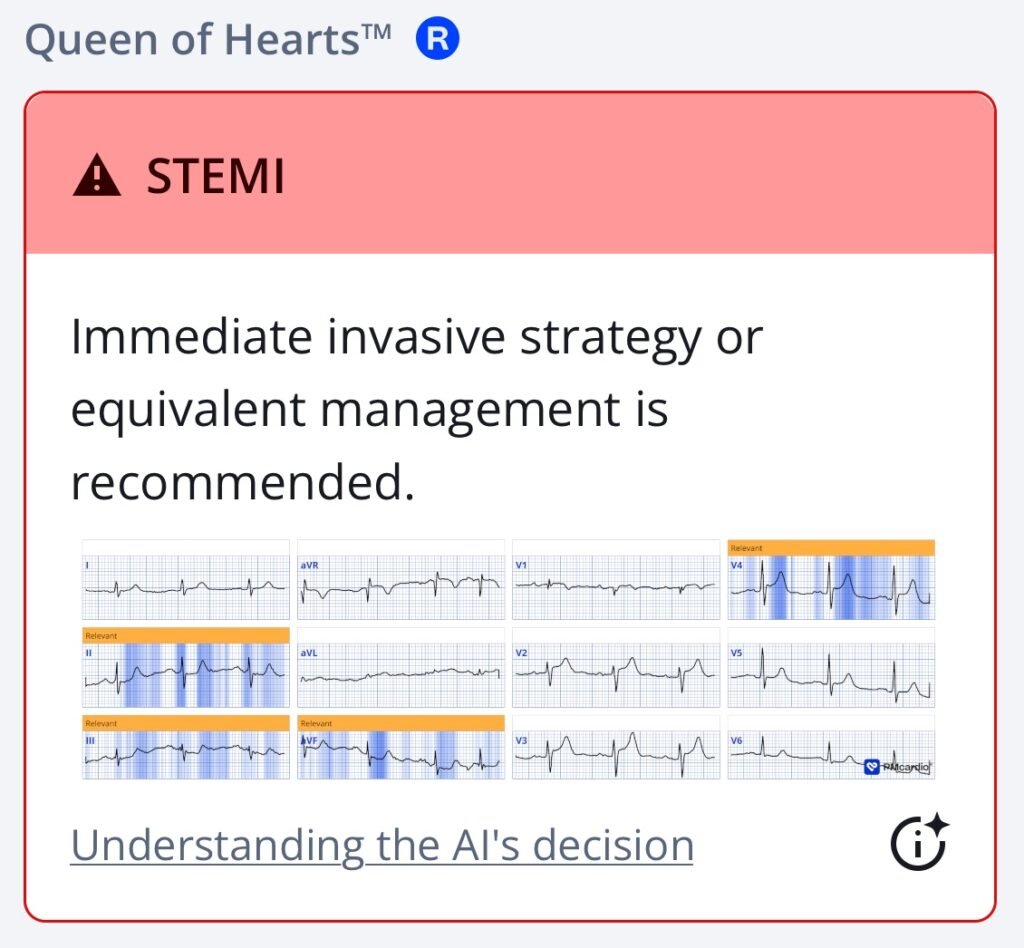
The Queen of Hearts algorithm highlights terminal T-wave abnormalities indicative of reperfusion. Whenever the AI model sees signs of reperfusion the adjudication of high-risk NSTEMI is given.
Smith: this is Wellens’ syndrome. It is spontaneous reperfusion of an LAD Occlusion that was not recorded on ECG at the time of occlusion. It requires resolution of chest pain and terminal T-wave inversion (Pattern A) which will evolve into deep symmetric T-wave inversion over a very variable time period (Pattern B)
Smith still: —-What are you worried about when there is Wellens’ syndrome? Re-occlusion!! There is an unstable thrombus in the LAD which can propagate and occluded at any time. Wellens is a “Transient OMI (transient STEMI)”. There are those who believe that transient OMI need not go emergently to the cath lab. This is foolish, as I discuss here: Chest pain, resolved. Does it need emergent cath lab activation (some controversy here)? And much much more.
And this further illustrates the problem (re-occlusion may be asymptomatic): Why we need continuous 12-lead ST segment monitoring in Wellens’ syndrome
The emergency department was overcrowded that day, and because the patient was pain free on arrival, he was seated in the waiting area. Shortly after arrival, chest pain recurred, and a repeat ECG was obtained.
The repeat ECG is shown below. What has happened?
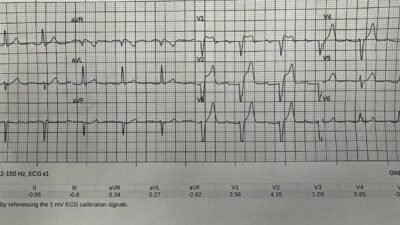
ECG #2 Recorded in the ED
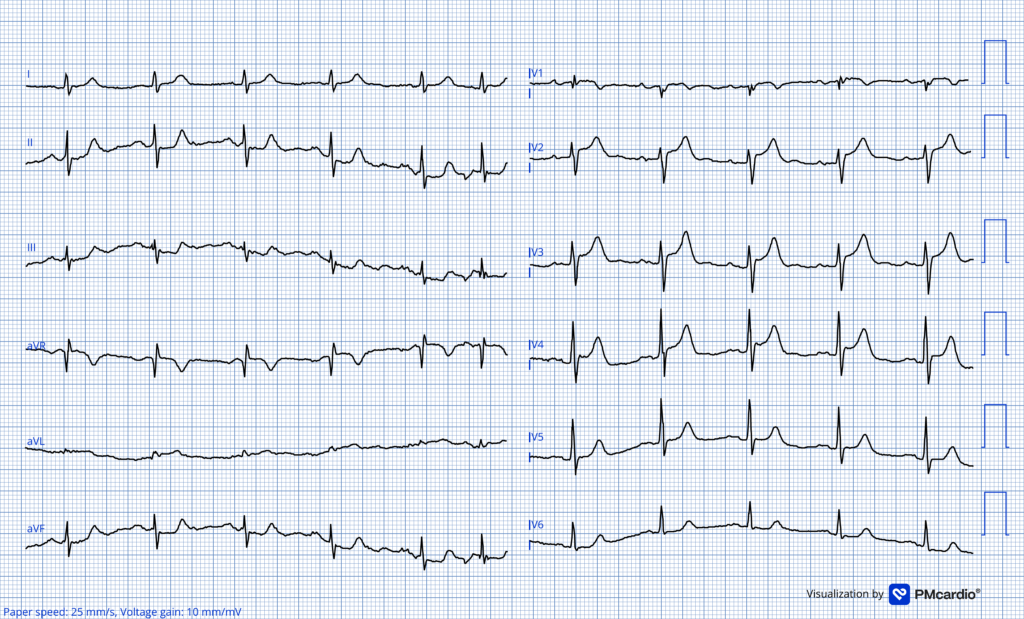
The T wave inversions have now disappeared and are replaced by hyperacute T waves. “Precordial swirl” pattern is noted along with proportionally significant STE in aVL and reciprocal ST depression in leads II, III and aVF. This ECG is diagnostic of proximal LAD occlusion before the first diagonal. The ECG barely meets STEMI-critera. Whenever recurrence of chest pain is accompanied by loss of T wave inversions one must think pseduonormalization. Pseudonomalization is OMI (re-occlusion) until proven otherwise. The Queen of Hearts identified this as OMI.
Sublingual NTG was administered again and 10 minutes after ECG #2 the patient became pain free once more. A repeat ECG was obtained after the monitor showed a change in the cardiac rhythm.
How do you put this ECG into clinical context?
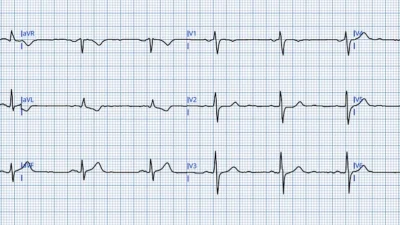
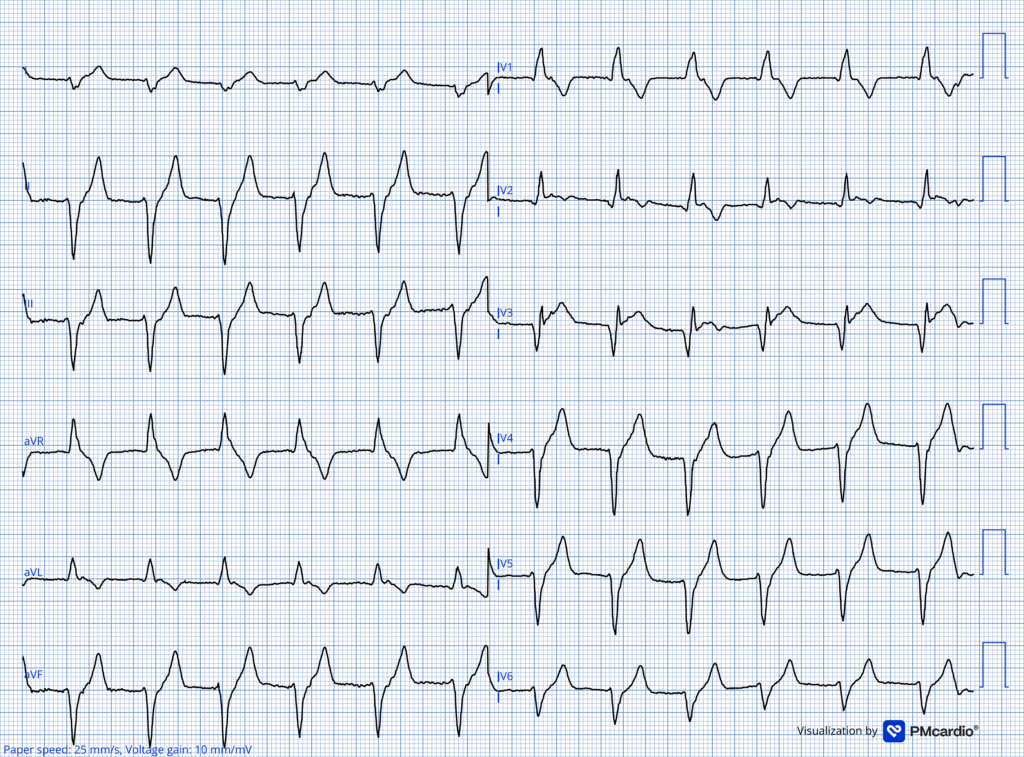
ECG recorded after rhythm change
What do you think?
This ECG demonstrates a regular wide-complex rhythm at approximately 80 beats per minute, consistent with an accelerated idioventricular rhythm (AIVR). It is too slow to be VT. There is a right bundle branch block and left anterior fascicular block–like QRS morphology; this shows that the beats originate in the left posterior fascicle. In lead V2, there is concordant ST-segment elevation with T-wave inversion.
AIVR is an arrhythmia most often seen as a reperfusion phenomenon. This patient had an extremely high-risk ACS presentation, with multiple episodes of chest pain and OMI features on the ECG, indicating a high risk of re-occlusion. He was transferred to a PCI-capable facility, where angiography demonstrated a critical LAD stenosis with TIMI III flow. Troponin T peaked at a modest 198 ng/L, and echocardiography showed a normal ejection fraction with a transient wall motion abnormality in the apical region of the left ventricle.
This post illustrates the dynamic nature of acute coronary syndrome, with the initial ECG showing early Wellens-type T-wave inversion, followed by pseudonormalization and development of OMI before a further episode of reperfusion manifested by transient AIVR. The post-PCI ECG (below) demonstrates typical evolution of reperfusion T waves, now consistent with Wellens Pattern B morphology.
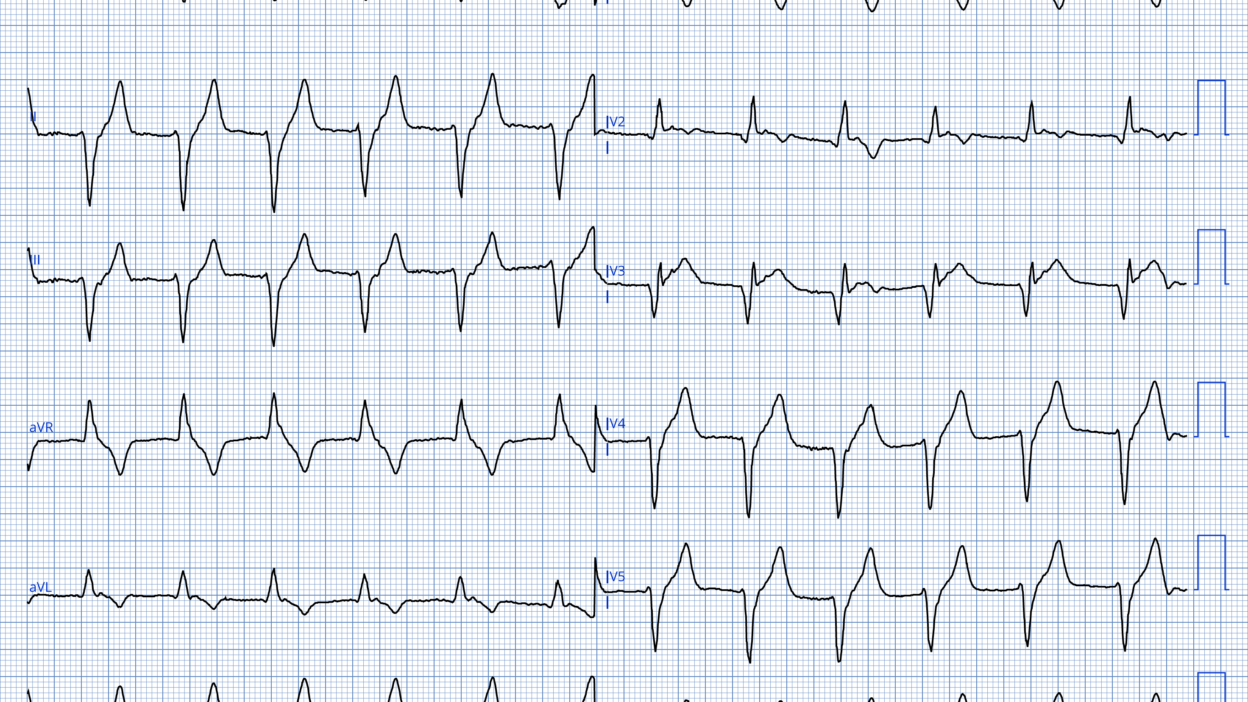
POST-PCI tracing
Wellens pattern B T wave inversion. This ECG was recorded the day after the PCI procedure.
QoH interpretation of ECG #2
Another great case (trops not ALWAYS positive in Wellens): Severe chest pain, resolved. Serial troponins nearly undetectable at 3 ng/L
Learning points:
- ACS is a dynamic process. T wave inversion or AIVR after recent chest pain is a favorable prognostic sign and signifies reperfusion.
- Recurrence of chest pain with disappearance of prior T-wave inversion represents pseudonormalization and should be considered OMI until proven otherwise.
- Reperfusion T waves typically deepen gradually after successful reperfusion, provided the culprit artery remains patent.
- T wave inversion must always be interpreted in clinical context. If there are ongoing ischemic symptoms, cath lab activation is warranted regardless of “reassuring” T-wave appearance.
- Terminal T-wave inversion due to reperfusion evolves into deep symmetric T-wave inversion over a variable time period
= = =
======================================
MY Comment, by KEN GRAUER, MD (4/2/2026):
Today’s case by Dr. Nossen provides a beautiful example of serial ECG changes that tell a story of repetitive “culprit” artery closure and reopening. Fortunately — these serial ECG changes were recognized by providers in today’s case, and promptly acted upon with timely cath and PCI.
- So insightful is the clinically correlated sequence of the 4 ECGs in today’s case — that I propose review of these 4 abbreviated tracings (that I’ve put together in Figure-1) as a time-efficient introduction for the uninitiated to the clinically relevant physiology of the OMI paradigm.
- Simple awareness that today’s patient contacted EMS for acute CP (Chest Pain) that resolves by the time ECG #1 is recorded — provides presumptive evidence of acute coronary occlusion as soon as this 1st tracing is seen (without the need to wait until ST elevation).
- Subsequent tracings tell us when the “culprit” artery has opened — and when it has reclosed.
= = =
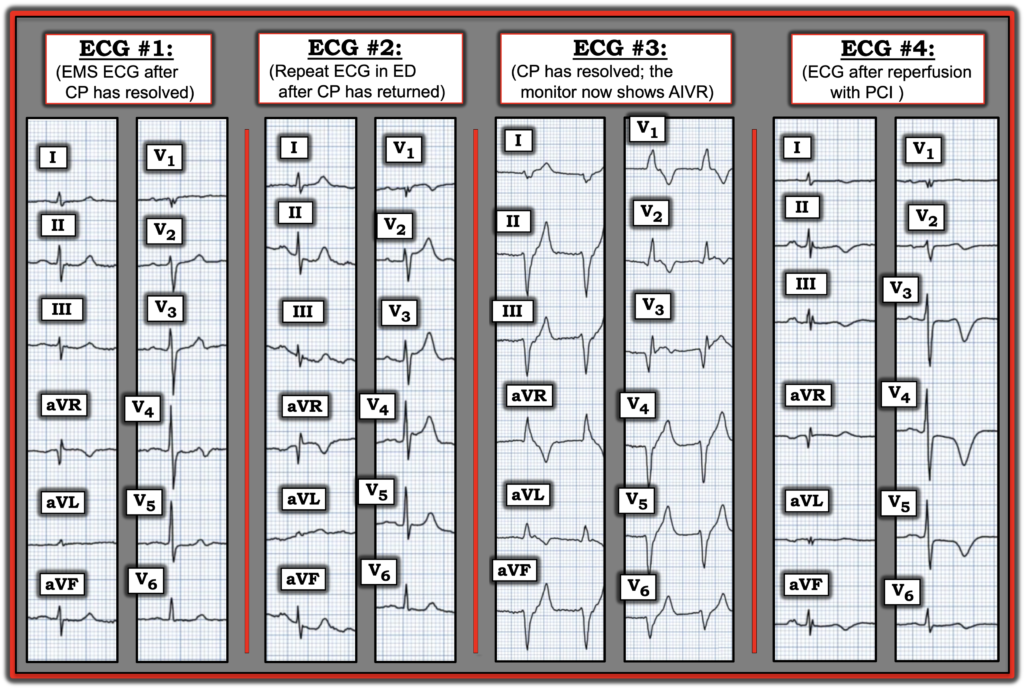
Figure-1: I’ve condensed today’s 4 sequential ECGs, accompanied by a 1-line relevant history. Doesn’t this Figure tell a story?
= = =
The Story inherent in Figure-1 …
- ECG #1: This is Wellens’ Syndrome. The patient contacted EMS for an episode of severe CP. By the time EMS arrived — his CP had lessened, totally resolving by the time ECG #1 was recorded. In this clinical context — the subtle up-down T waves in leads V3,V4,V5 are diagnostic of acute LAD occlusion that has now reperfused.
- The patient’s history of recurrent short-lived episodes of CP in the days prior to contacting EMS — are almost certain indication of repetitive LAD closures followed by spontaneous reopening of this “culprit” LAD artery.
- Simple correlation of this history in the context of ECG #1 clearly portrays a high-risk situation in need of prompt cath with PCI to prevent the large infarction that will probably occur if the warning conveyed by these multiple self-resolving CP episodes is not heeded.
- ECG #2: As per Dr. Nossen — the terminal T wave inversion of Wellens’ Syndrome has been replaced by enlarging positive chest lead T waves and worrisome downsloping inferior lead reciprocal ST depression. In the clinical context of the return of CP — ECG #2 is clearly telling us that the “culprit” LAD has reclosed!
- ECG #3: The rhythm is now AIVR (Accelerated IdioVentricular Rhythm). The occurrence of this rhythm in the clinical context that the CP experienced at the time ECG #2 was recorded has now resolved — tells us that there once again has been reperfusion (and that the LAD has again reopened).
- Note that despite this ventricular rhythm — frank ST elevation is seen in lead V3 of ECG #3.
- ECG #4: This is the ECG after PCI. The patient is pain-free — and the deep, symmetric T wave inversion in the LAD distribution of this tracing provides ECG evidence of clinical reperfusion following a successful PCI procedure.
= = =
Additional Learning Points:
- Clinical correlation of today’s history, interpreted in the context of ECG #1 — allows immediate recognition of a very high-risk critical LAD lesion in need of prompt cath with PCI as soon as this initial ECG is seen.
- There is no need to delay prompt cath because you are waiting for ST elevation to occur. Doing so risks the occurrence of a large infarction.
- If we “listen” — Clinically correlated serial ECGs will often tell us when the “culprit” artery is open, and when it has reclosed (as is illustrated in today’s case).
- The simple step of writing down on each serial ECG whether CP is present at the time that ECG is recorded (and if so — relative CP severity on a scale of 1-to-10) — allows us to develop a story of what is happening (thereby expediting our recognition of acute coronary occlusion — often without the need to delay intervention by waiting to see if ST elevation occurs).
= = =
= = =