Written by Magnus Nossen
I was reviewing a patient’s prior ECGs for an ongoing study when I came across the tracings from today’s case. The patient is a man in his 70s with a history of abdominal aortic aneurysm repair, hypertension, and mild COPD.
He had been experiencing intermittent palpitations for several weeks, and when his symptoms recurred, he contacted his primary care physician. He was found to be tachycardic, but apart from a heart rate of about 150 bpm his vital signs were unremarkable. He was referred to the emergency department, where the ECG below was obtained. No prior ECG was available. How would you interpret this ECG?
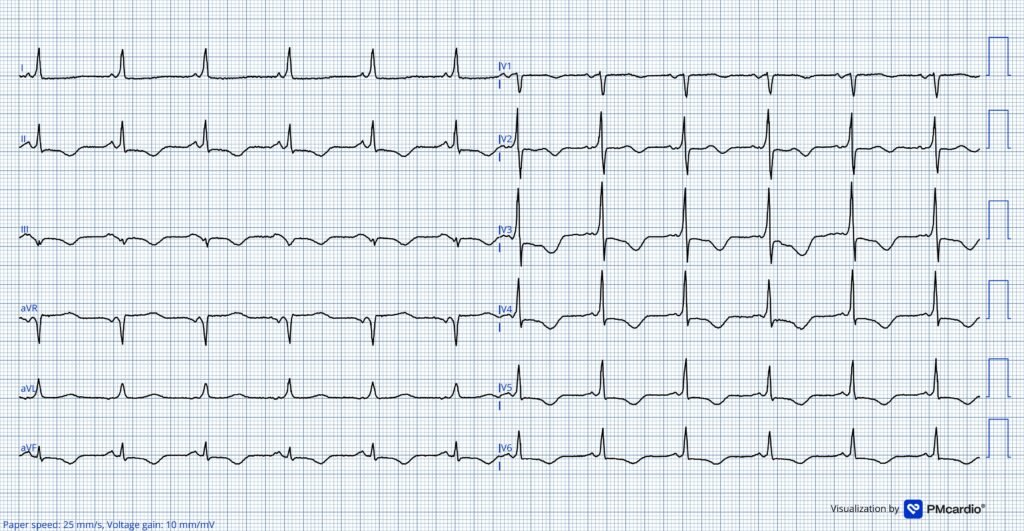
ECG # 1 recorded in the ED

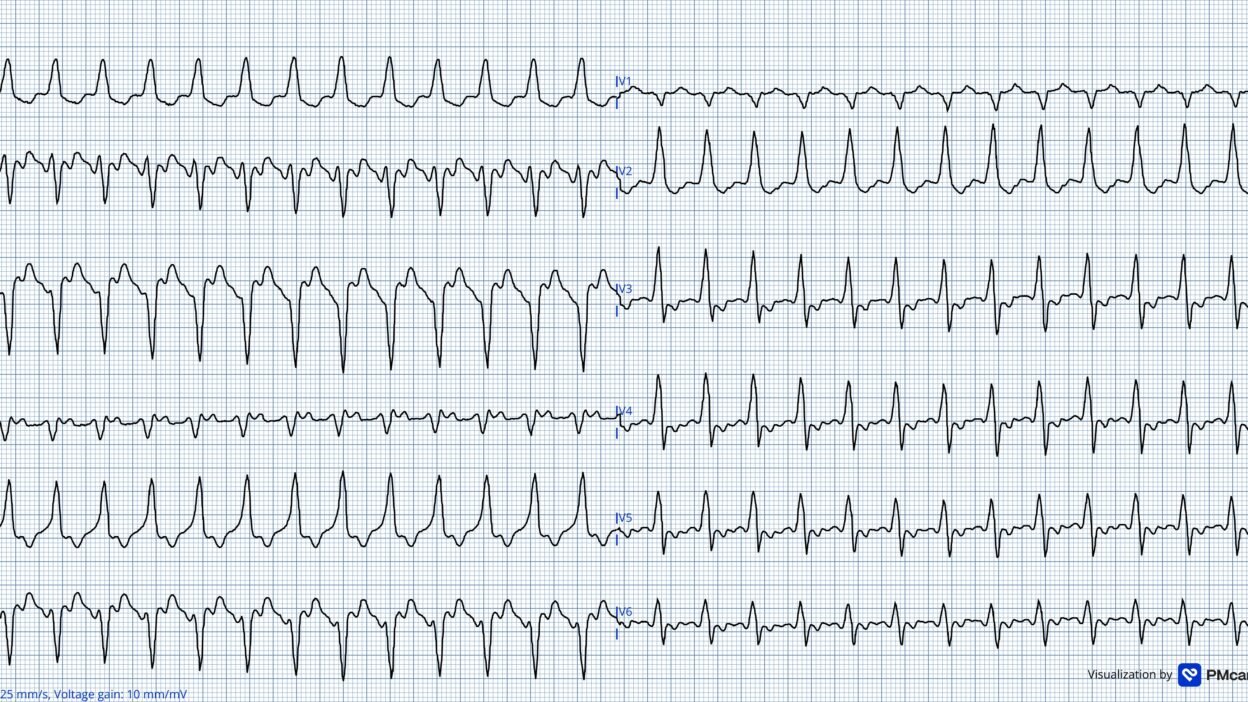
The ECG in today’s case shows a wide-complex tachycardia with a rate of 146 bpm and a QRS duration that is a bit difficult to assess, but it is at least > 130 ms. The QRS morphology is not consistent with any typical bundle branch block pattern.
The patient was stable; this gives you time to think and work through a structured diagnostic approach. How would you proceed with you diagnostic work up?
There are several medications and maneuvers that can help differentiate the causes of a regular tachycardia. A WCT can be either ventricular in origin or supraventricular with preexisting block or rate-related aberrant conduction. (Smith: additionally, of course, wide complex can be due to Hyperkalemia or Na channel blockade). If the WCT is due to a re-entrant supraventricular tachycardia with an associated conduction abnormality causing QRS widening, interventions that affect vagal tone or AV nodal conduction may be both diagnostic and therapeutic by interrupting the re-entrant circuit.
If atrial flutter is the underlying rhythm, these same medications or maneuvers may be diagnostic by revealing flutter waves, but will not necessarily terminate the arrhythmia.
My thoughts: When I saw ECG #1 — I thought the QRS morphology was consistent with ventricular origin of the arrhythmia. Then I noticed lead II, which I felt quite sure showed atrial activity at twice the ventricular rate. Lead aVL also caught my eye having a very slow initial R wave upstroke.
This slow initial ventricular activation would be unusual with 2:1 AV conducted flutter. In 2:1 AV nodal conduction — the conduction system is involved from the start of ventricular activation and the initial QRS upstroke is usually not this slow.
- This ECG just got much more interesting! How could we possibly explain very slow initial ventricular activation in lead aVL and the 2:1 AV conduction?
Figure 1

Figure 1 showing excerpt of lead II and lead aVL from the initial ECG. Vertical blue arrows point to atrial activity in lead II. Orange arrows point to very slow initial ventricular activation in lead aVL.
I could think of no other possible explanation other than that the rhythm was atrial flutter with 2:1 conduction over an accessory pathway. That said, it would seem that preexcitation should have been noted before in this 70 year old male with multiple hospital visits.
- I looked into the chart to see what had happened on this visit. The patient was admitted to the cardiology ward. No diagnostic maneuvers or medication was tried. I would have considered applying Lewis leads to try to visualize atrial activity better. If that had not helped, I would have tried to obtain a transesophageal ECG. Neither was done.
The patient was admitted with telemetry monitoring. The heart rate remained stable throughout the night. The next day the cardiologist interpreted the rhythm as 2:1 atrial flutter. No comment on the QRS morphology was made. A TEE was performed, which ruled out atrial thrombus. The patient was subsequently cardioverted.
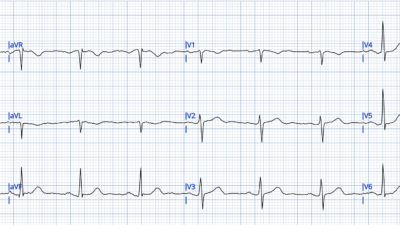
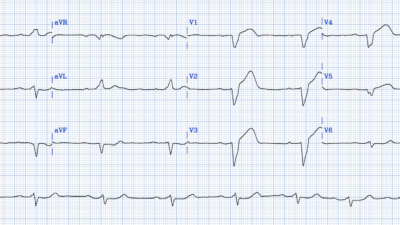
ECGs obtained after cardioversion
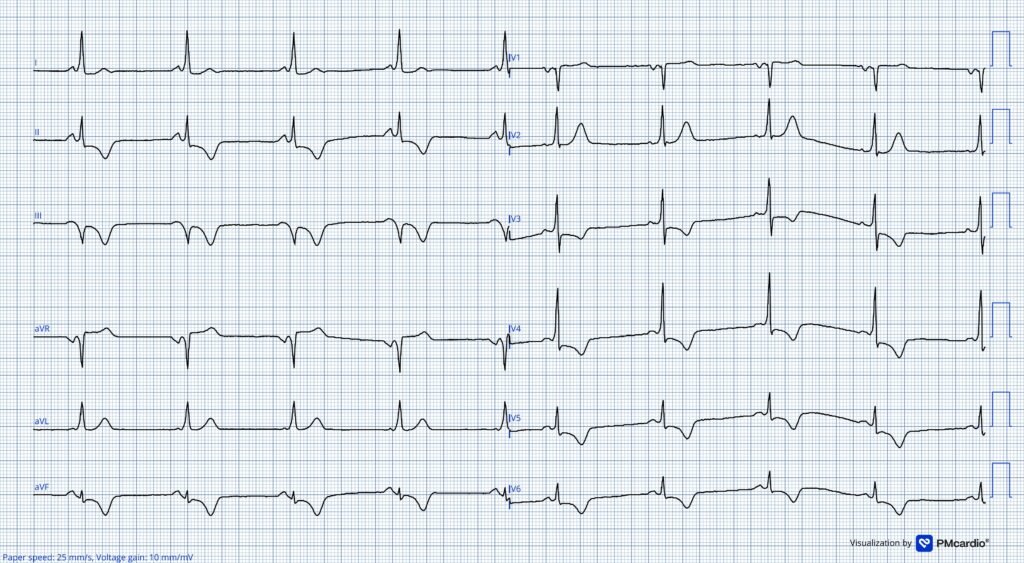
Both of the above ECGs show clear pre-excitation. Delta wave polarity, QRS axis and R/S wave transition is similar to the intitial ECG.
These two ECGs show clear pre-excitation, making the initial tracing diagnostic of 2:1 atrial flutter conducted over an accessory pathway!
Quite surprisingly, the pre-excitation pattern was not commented on! The patient was started on amiodarone and referred for catheter ablation of atrial flutter.
- In the period leading up the the ablation procedure he was admitted for recurrence of palpitations.
- Of note, the amiodarone slowed the atrial flutter rate.
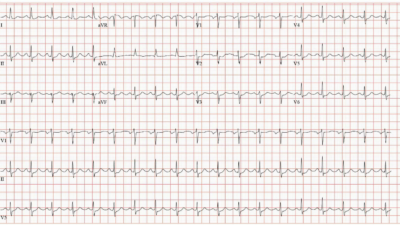
- The ECG below was recorded at one of these visits, and now shows narrow QRS complexes. As the flutter cycle length increased, the AV node was able to conduct in a 2:1 pattern, resulting in a narrow QRS at the slower flutter rate.
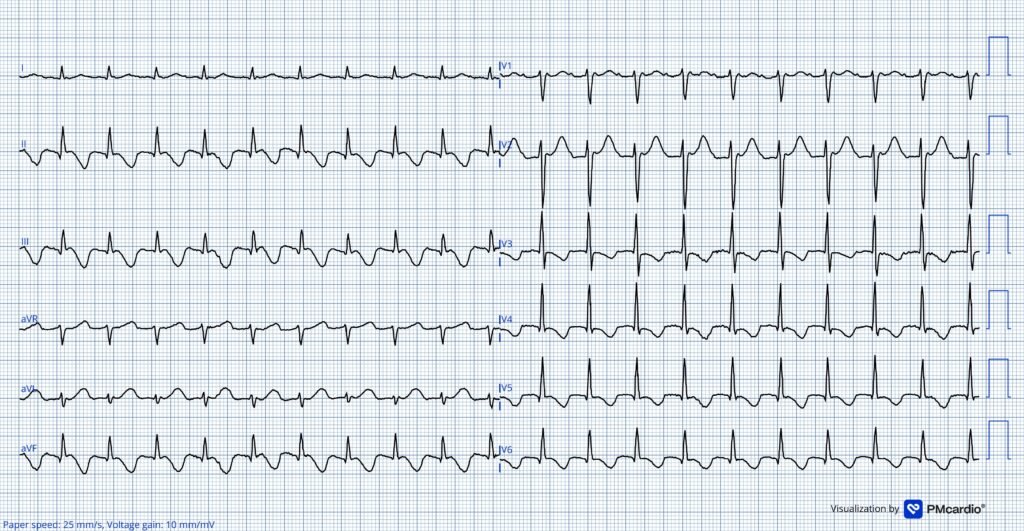
In this ECG there is an atypical flutter with 2:1 AV conduction (the ECG at the top was 2:1 conduction through the accessory pathay, since the flutter was too fast for the AV node at that time). The ventricular rate is ~120 beats per minute. The atypical flutter is evident by the pseudo r’ seen in lead V1.
In adult and elderly patients, the AV node may exhibit progressively increased PR intervals at higher heart rates. This rate-dependent AV nodal delay can allow the electrical impulse to preferentially conduct over the accessory pathway, which has faster conduction velocity. This phenomenon explains why preexcitation may become more apparent with increasing heart rates.
- This likely accounts for why the initial ECG demonstrated a preexcitation pattern at a heart rate of 146 bpm, while narrow QRS complexes were observed in the ECG above at a lower heart rate. At the slower rate, AV nodal conduction remained sufficiently rapid to depolarize the ventricles before the accessory pathway contribution became manifest.
- Another possible explanation is that the electrical impulse is activating the AV node in retrograde fashion, rendering it refractory to the antegrade flutter wave. This would favor conduction exclusively down the accessory pathway.
= = =
Addendum: Adenosine can be used to unmask flutter waves in 2:1 conducted flutter. However, in today’s case — had adenosine been given for diagnostic purposes, there would have been no unmasking of flutter waves as impluses would still conduct over the accessory pathway.
The patient eventually underwent an electrophysiological procedure in which typical and atypical atrial flutter rhythms were documented. An ablation procedure for typical atrial flutter and pre-excitation was successfully performed.
Learning Points:
- Increasing pre-excitation may be seen at faster heart rates if the AV node shows rate dependent PR prolongation.
- Pre-excitation can be intermittent, may remain asymptomatic, and is sometimes first recognized in middle-aged or elderly adults.
- In the rare instance of 2:1 atrial flutter with conduction over an accessory pathway — Adenosine will not unmask the underlying flutter.
= = =
======================================
MY Comment, by KEN GRAUER, MD (5/10/2026):
I found today’s case by Dr. Nossen to be a fascinating illustration of an arrhythmia phenomenon that I had not previously seen. On reviewing this case — I’d add the following Learning Points to Dr. Nossen’s excellent discussion:
- Sherlock Holmes (the amazingly astute fictional detective created by Sir Arthur Conan Doyle) is known for saying, “When you have eliminated the impossible — you are left with the improbable”.
- Applied to the world of complex arrhythmia solving — this translates to, “thinking outside of the box” when confronted with a highly unusual arrhythmia that does not obey the usual rules. This is precisely what Dr. Nossen does in today’s case — which is why he considered a possibility that neither he nor I had ever before seen (and which was overlooked by other cardiologists on the case).
- When you are left with postulating an unusual but possible explanation for an otherwise seemingly unsolvable arrhythmia — Consider ways you can go about validating your “out-of-the-box” theory. In today’s case (since no prior ECG was available at the time the patient presented to the ED) — Dr. Nossen contemplated: i) Using Lewis Leads (See My Comment at the bottom of the page in the November 23, 2025 post for details regarding use of Lewis Leads) — or — if Lewis Leads were not successful, attempting placement of a transesophageal ECG; — ii) Searching the patient’s chart for previous ECGs, antiarrhythmic medications tried, and/or other information regarding known arrhythmias that the patient has had; — and, iii) Consideration of synchronized Cardioversion (which when ultimately performed, converted the patient to sinus rhythm — which revealed the “telltale” delta waves of WPW).
- Look to pathophysiology for support of your theory (As noted by Dr. Nossen — increasing preexcitation may at times be seen at faster heart rates, as occurred during the WCT rhythm with 2:1 AFlutter).
- Finally — “Rules are made to be broken”. Although most patients with WPW who develop symptomatic arrythmias do so by middle-age — today’s case involves a 70-something man who despite a number of underlying medical and cardiac conditions, apparently never before had WPW-related cardiac arrhythmias despite clear evidence of WPW on today’s tracings. AP (Accessory Pathway) conduction induced by rapid heart rates may be seen for the 1st time at any age.
= = =
Applying the above Learning Points to Today’s CASE:
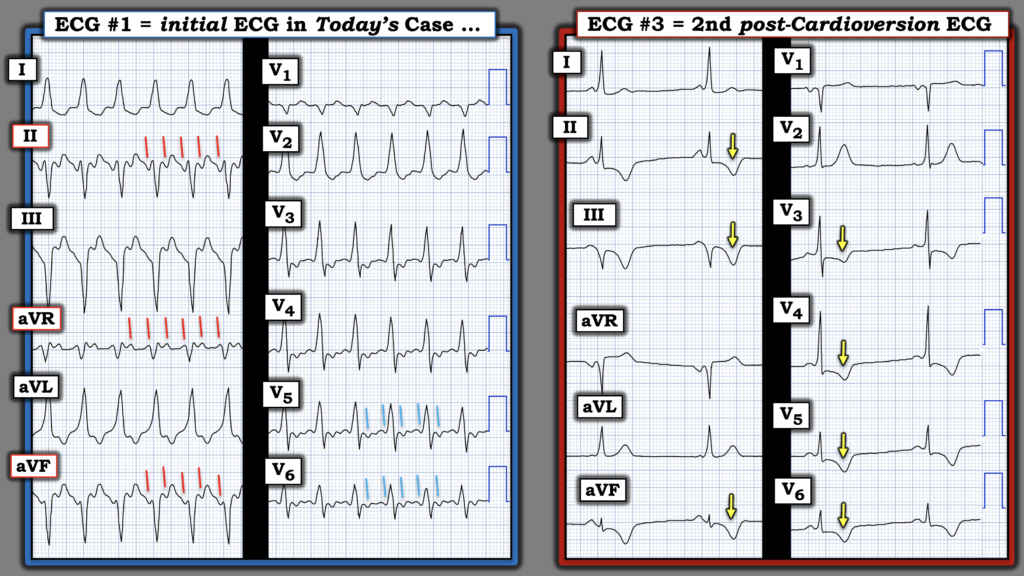
For clarity in Figure-1 — I illustrate my thoughts regarding today’s initial ECG, by comparison with the 2nd post-cardioversion ECG.
- The initial ECG in today’s case (LEFT tracing in Figure-1) — represents a regular WCT (Wide-Complex Tachycardia) at a rate just under 150/minute — without clear sign of sinus P waves.
- The usual differential diagnosis includes: i) VT (Ventricular Tachycardia); — ii) A reentry SVT (SupraVentricular Tachycardia), most commonly AVNRT or AVRT; — and, iii) AFlutter (Atrial Flutter) — with Sinus Tachycardia and Atrial Tachycardia being much less common causes given the above description of today’s initial rhythm.
- As per Dr. Nossen — the fact that QRS morphology in ECG #1 does not resemble any known form of conduction defect raises the possibility of VT (ie, The QS in lead V1 and lack of S waves in leads I,aVL is against RBBB conduction — and the early transition with predominant R wave already by lead V2 rules out LBBB conduction).
- The above said — precise 2:1 atrial activity is seen in 3 of my “Go-To” leads (slanted RED lines in Figure-1) — which at the ventricular rate of ~150/minute, strongly suggests there is underlying AFlutter (See My Comment at the bottom of the page in the 9/21/2025 post regarding my “Go-To Leads” when looking for AFlutter). The slanted BLUE lines in leads V5,V6 also show the 2:1 atrial activity of AFlutter.
- Note: It is possible for AFlutter and VT to simultaneously exist — but this phenomenon is exceedingly rare (Curtis AB, Grauer K — J Fam Prac 30:706-710, 1990 — and— Anderson, Rubin — Am H J 56(2):299-303, 1958).
= = =
BOTTOM Line: Mystery solved with successful cardioversion to sinus rhythm. As seen in the 2nd post-Cardioversion ECG (RIGHT tracing in Figure-1) — upright sinus P waves are now clearly seen in lead II.
- The PR interval in ECG #3 is short — and subtle delta waves are seen in many of the leads (best seen in leads I,aVL; V2,V3,V4 — with negative delta waves seen in leads III and aVR).
- It’s important to appreciate that the relative amount of preexcitation that may be seen with WPW may vary. Perhaps the reason that cardiology failed to notice the appearance of WPW on the post-cardioversion tracings — is that the QRS is narrow, the PR interval looks normal in lead II, and delta waves are subtle because there is only partial preexcitation in ECG #3.
- KEY Point: As emphasized by Dr. Nossen — increasing preexcitation may be seen at faster heart rates — and the heart rate in ECG #3 has markedly slowed since the WCT in ECG #1. That said — QRS morphology in ECGs #1 and #3 looks similar in many leads, with the exception that the QRS has significantly narrowed at the slower rate after cardioversion.
- Final Thought: Note the deep T wave inversion in multiple leads of the post-conversion tracing! (YELLOW arrows in Figure-1). This is almost certain to represent a “Memory” effect following the sustained tachycardia prior to cardioversion. It is not due to ischemia.
= = =
Figure-1: Comparison between today’s initial ECG — and the 2nd ECG obtained following cardioversion (To improve visualization — I’ve digitized the original ECG using PMcardio).
= = =
= = =