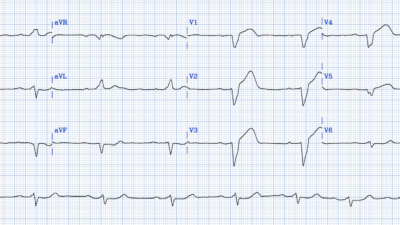
A 50-something man had onset of chest pain which then resolved. About an hour later, the chest pain recurred and he went to the ED. Approximately 30 minutes after onset of chest pain, this ECG was recorded. (It was sent to me with no information.)
What do you think?
The sender had this interpretation:
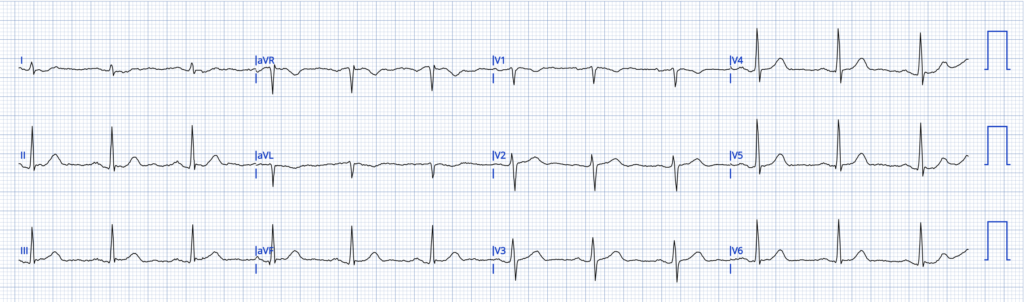
“Early inferior OMI? I feel like the ST elevation is pretty subtle, but then there is the T-wave inversion in aVL and lead I. I feel like in aVL it doesn’t mean as much because the QRS is also negative, but how about lead I? That has an upright QRS and inverted T wave and some ST depression.”
My response: “I agree that it is very suspicious, but I also agree that it is not diagnostic. Very tough one. Keep getting serial EKG‘s. I will run it through the queen of hearts.” I also thought: I am particularly worried about that ST depression in lead I, with a down-up T-wave.
I showed this to my “EKG Nerdz” message group without any information and they all called it OMI.
Comment: the QRS axis is exactly 90 degrees (toward aVF and perpendicular to lead I). For this reason, in aVL, the QRS is negative, as is the T-wave. Therefore, the negative T-wave in aVL is of lower significance that it would otherwise be. In lead I, however, the QRS is isoelectric (as much positive as negative) and so the T-wave should be upright, and the ST should also be isoelectric. However, the ST is down and T-wave down-up.
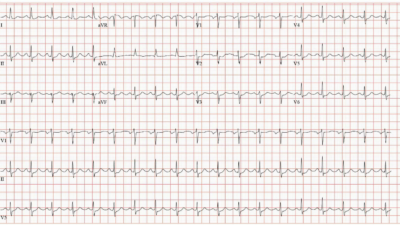
The PMCardio Queen of Hearts AI ECG Model interpretation:
Notice the Queen also recommends serial EKGs every 15-20 minutes.
No repeat ECG was recorded.
Case continued:
A troponin was drawn 10 minutes after the ECG (45 minutes after recurrence of chest pain): it returned at 11 ng/L (URL for this Siemens Atellica assay is 53 ng/L). A 2nd troponin was drawn one hour later and returned at 34 ng/L. There was no repeat ECG. For this assay, a one hour delta > 12 ng/L (in this case it is 23 ng/L), is all but diagnostic for acute MI, as below:
Based on the European Society of Cardiology (ESC) 0/1-hour protocol, this patient has a 69.4% to 75.6% probability of an adjudicated acute myocardial infarction (AMI). The patient’s presentation results fall directly into the Rule-In Zone due to an absolute troponin change that exceeds validated diagnostic thresholds. The probability of acute myocardial injury is higher, at 95.7%. In the context of acute chest pain, any myocardial injury is acute MI until proven otherwise.
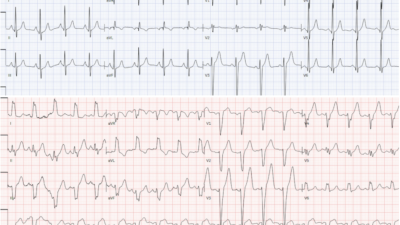
The patient was off monitor. At approximately 2 hours after arrival, the patient was found unresponsive and pulseless. He was found to be in ventricular fibrillation. Resuscitative measures were futile.
Was this arrest due to acute OMI? Almost certainly, though can’t be proven. 1. A suspicious presentation, 2. VERY suspicious initial ECG, 3. rising troponin diagnostic of MI, then 4. ventricular fibrillation.
I showed this ECG without any information to a very well trained community emergency physician. He said that he would put the patient in the waiting room.
After I told him what happened, he agreed that an ECG every 15 minutes is essential.
Learning Points:
- Always put chest pain patients with persistent pain on a monitor.
- Learn to recognized subtle signs of possible OMI.
- Always get serial ECGs whether subtle signs are present or not.
- Any rising troponin in a chest pain patient is myocardial infarction until proven otherwise.
Ken has many other important points below.
= = =
==================================
MY Comment, by KEN GRAUER, MD (5/13/2026):
I always try to look at cases like this one before I read ahead to see what happened to the patient. As a result — My Comment below is based on my impression of today’s initial ECG, knowing only the brief history presented in Dr. Smith’s opening paragraph. In this way — I can be more objective in my review of the ECG findings — because, “hindsight is 100% accurate in the retrospectoscope” (ie, It’s EASY to comment in retrospect when you already know the answer as to what happened to the patient).
- The Clinical Reality: Most (if not all) of us have learned from the painful experience of being assigned to a patient who seemed “OK” — but while waiting for a room in a crowded ED (Emergency Department) — the patient suddenly codes and dies before being fully evaluated.
- As a result — We need to learn from cases like this one. I therefore focus My Comment on reinforcing the important Learning Points highlighted above in Dr. Smith’s discussion.
= = =
— What Went Wrong? —
We learn from going back to case specifics — and soul-searching as we contemplate what might be done differently the next time around.
i) The HISTORY was not fully appreciated …
- The 50-year old man in today’s case had an episode of new CP (Chest Pain) — that then resolved — but then recurred an hour later, prompting his visit to the ED.
- It’s common during the evolving process of an acute event — for the “culprit” artery to spontaneously reperfuse. When this happens — the patient’s CP goes away (or at least decreases) — and ECG indicators of acute ischemia may largely (or even totally) resolve.
- The problem is that an unstable plaque may then at any moment spontaneously reocclude — which is typically marked by return of CP and return of the ECG abnormalities.
- Somewhere in between the process of acute coronary occlusion (which is marked by ST elevation) and spontaneous reperfusion (marked by ST depression and T wave inversion) — an ECG pattern known as “pseudo-normalization” may be seen, in which the ECG may look almost normal.
- Because the history in today’s case potentially “fits” with the above scenario — providers need to be aware of the very subtle ECG abnormalities that might be seen if the initial ECG is recorded during the pseudo-normalization stage.
ii) Troponin may not be elevated early on …
- The 1st (and even the 2nd) hs-Troponin may not necessarily be elevated despite an acute OMI. This is especially true if the period of acute coronary occusion is brief — as seemed to occur in today’s case, in which the patient’s initial CP episode spontaneously resolved.
- In a patient with worrisome symptoms — any elevation of Troponin (even a very small one) is significant.
- On occasion — the first 2 Troponin values may both fall within the URL (Upper Reference Limit) — without these values necessarily indicating a normal result. As discussed by Drs. Smith and McLaren in the March 24, 2023 post — if the delta (ie, change) in serial Troponins is significantly increasing (and the Troponin delta in today’s case more than doubled from 13 to 33 ng/L for the 2nd Troponin done just 1 hour later) — then this increasing delta value should be taken as an abnormal result.
iii) ECG Abnormalities may be Subtle …
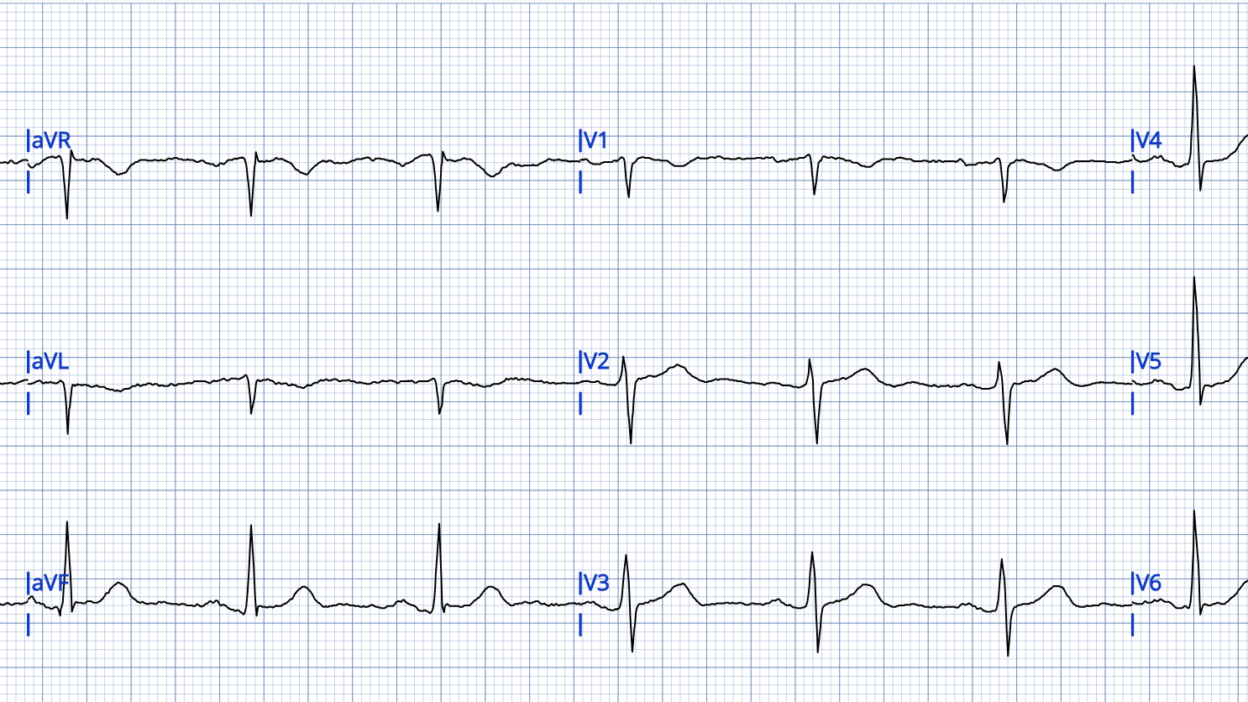
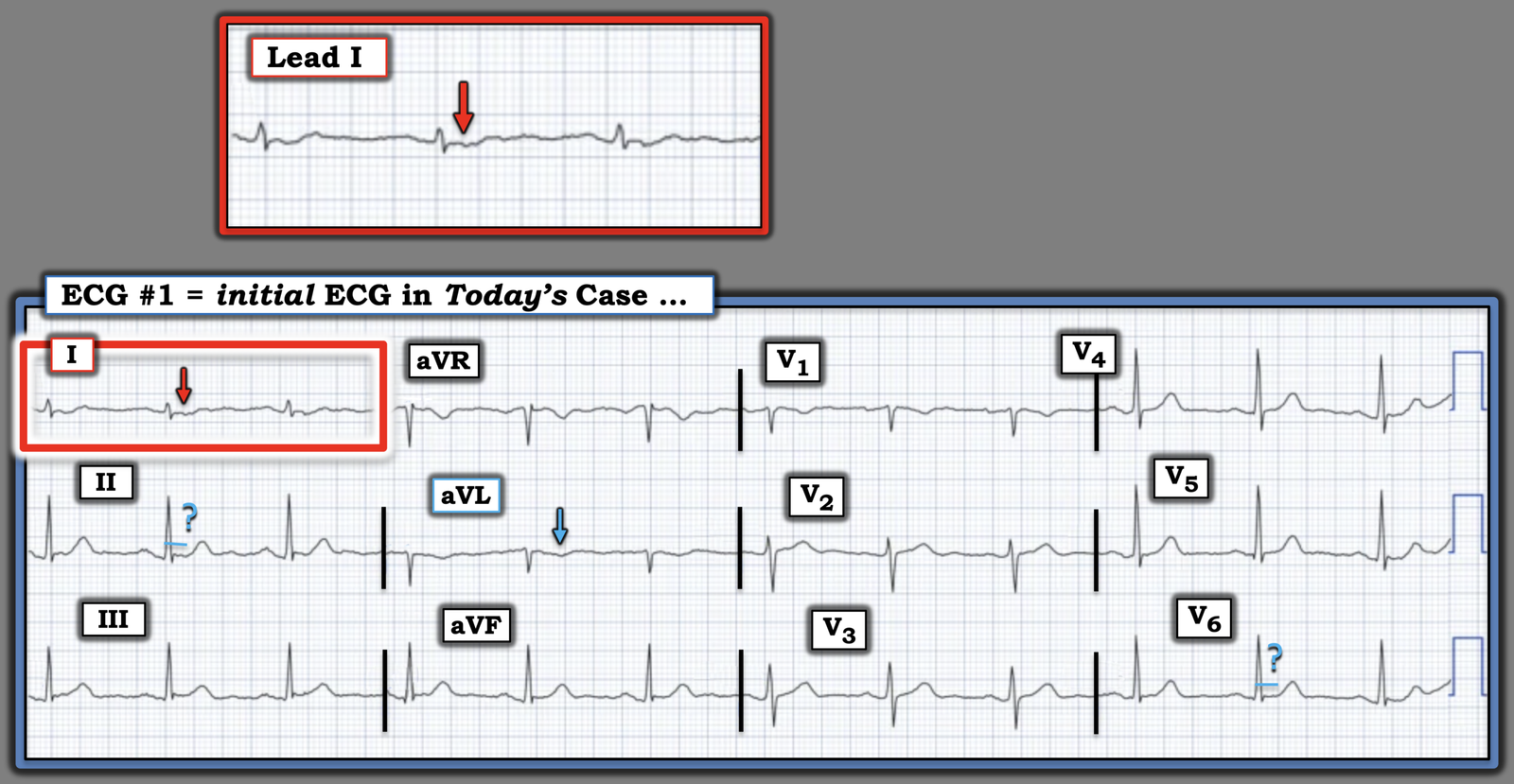
For clarity in Figure-1 — I’ve repeated and labeled today’s ECG.
- The rhythm is sinus. All intervals (PR,QRS,QTc) and the frontal plane axis are normal. There is no chamber enlargement.
- There are no Q waves — and R wave progression is normal.
- I’ve highlighted several subtle ST-T wave abnormalities (ie, some ST segment straightening in leads II and V6 — and T wave inversion in lead aVL) — but these are nonspecific (and non-diagnostic) changes about which no definite conclusion can be reached (I thought the base of the inverted T wave in lead aVL was a bit wider-than-expected given small size of the QRS in this lead — but still non-diagnostic).
- The above said, my “eye” was immediately drawn to the ST-T wave in lead I (within the RED rectangle). My overall impression of this tracing was identical to that of the clinician who submitted today’s case, and to that of Dr. Smith and of our EKG Nerdz colleagues ==> Despite non-diagnostic ST-T wave morphology in 11/12 leads — the ST-T wave in lead I just should not look like this!
- For clarity in Figure-1 — I’ve magnified lead I, which although there is some artifact distortion with some variation in ST-T wave detail — each of the 3 complexes in lead I show ST segment flattening with slight ST depression.
- Shape counts more than the amount of ST deviation in this tracing (especially given tiny size of the QRS in lead I).
- Bottom Line: As per Dr. Smith — Although ECG #1 is non-diagnostic — it is a highly suspicious tracing when considered in the context of the clinical history (with today’s patient potenially presenting to the ED during a period of time that might correspond to the “pseudo-normalization” phase) — especially given the increasing Troponin delta.
= = =
Figure-1: I’ve labeled the initial ECG in today’s case.
= = =
— What to Do? —
The answer is simple: When uncertain about whether your patient is (or is not) “in process” of acutely evolving an OMI:
- Repeat the 1st ECG within 10-20 minutes. Continue repeating the ECG frequently thereafter until the need for prompt cath can be confidently established (or until the point when you know prompt cath is not needed).
- Echo at the bedside (as a localized wall motion abnormality would establish the need for prompt cath).
- Continued CP in association with an abnormal Troponin is indication for prompt cath.
- And, in the meantime (as per Dr. Smith) — Keep the patient on a monitor!
= = =
= = =