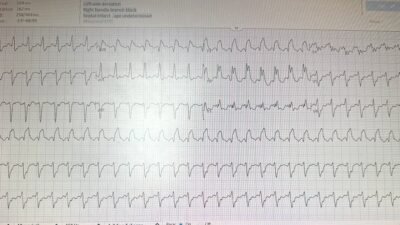
A man in his mid 50s was playing soccer and collapsed. Bystanders initiated CPR and delivered 3 AED-advised shocks. The patient was intubated by EMS and transported to the emergency room via ambulance. The note describes agonal respirations with fixed and dilated pupils (more on this later). Upon arrival, the following ECG was obtained:
What do you think?
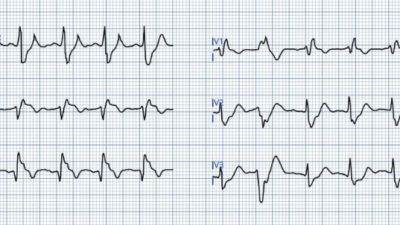
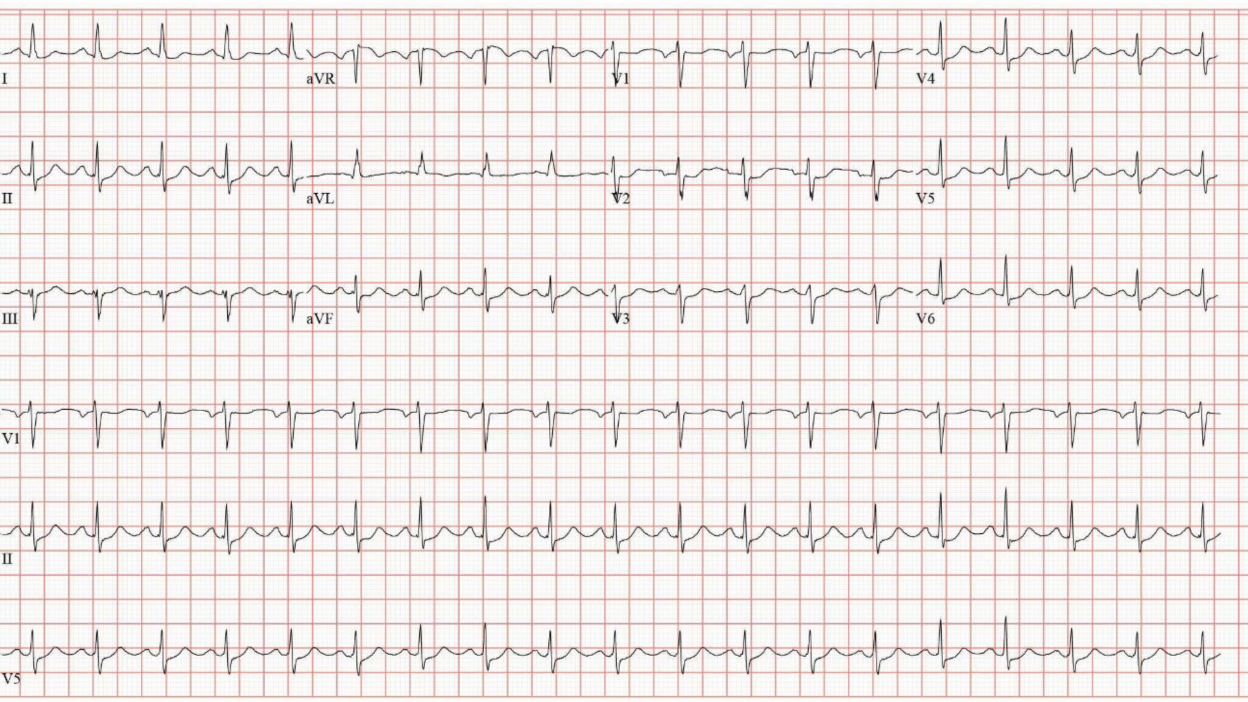
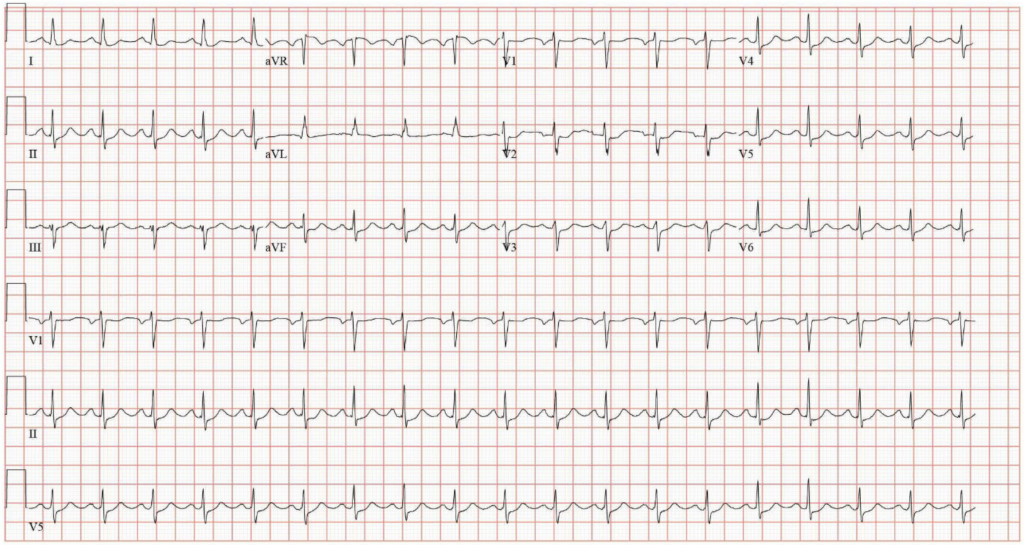
On the one hand, this ECG could be considered quite subtle. But on the other hand, this is an extremely suspicious situation — VF arrest (assuming AED shock was appropriately indicated) during exertion. Anyone looking at the ECG should be able to see that there is SOME ST depression in the precordial leads. That is already enough to begin suspecting and defending against OMI. On my inspection (and others may disagree), the precordial lead with maximal ST depression is V4, a finding which is diagnostic for posterior OMI. Queen of Hearts also diagnoses OMI with low confidence. There is very limited documentation, but repeat ECG almost 2 hours later is shown below.
This ECG should be obviously diagnostic to almost anyone, and was immediately recognized as a STEMI. In response, the emergency physician initiated transfer to a PCI capable facility.
Smith: a 2 hour delay leads to unacceptable myocardial loss.
Upon arrival there, the first two high sensitivity troponin I (hsTnI) values had resulted: first 58 ng/L, then 13,557 ng/L (reference: < 35). Thus, as expected, there is already a lot of myocardial loss.
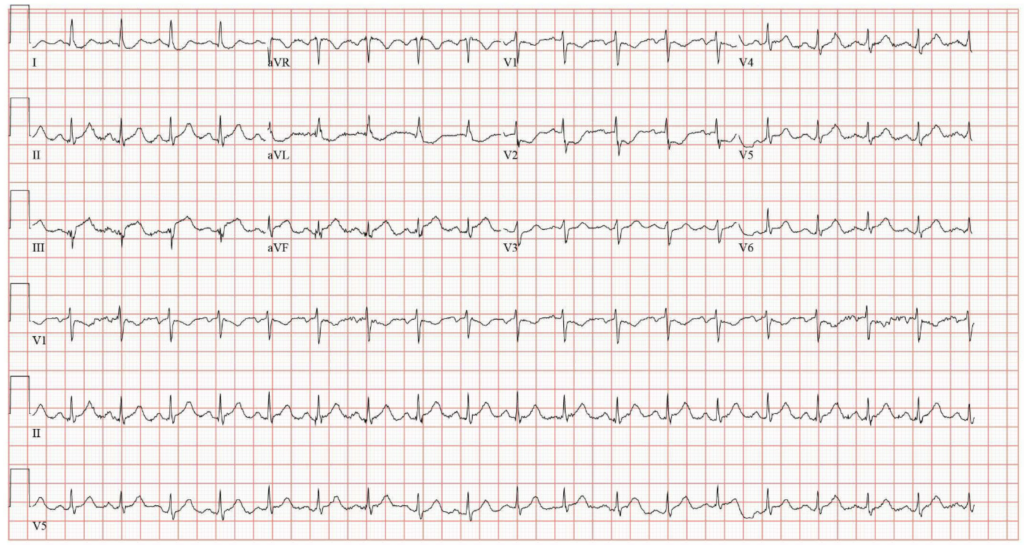
The documented plan is coronary angiography that evening. This did not happen. HsTnI continued to rise. Repeat ECG two hours later showed reperfusion.
The following day (after completion of the infarct with peak hsTnI 26,263 ng/L), the cardiology note again indicated a plan for heart catheterization which did not occur for reasons that were not documented, but may relate to the documentation the next day.
On hospital day 3, the patient remained intubated but was following commands when sedation was lightened. The interventional team did not feel that catheterization was indicated without formal consent, and no surrogate had been identified at that point. In addition to defying common sense, there is guideline support for intervention in emergency situations when informed consent is unable to be obtained.
- 2021 SCAI expert consensus statement (endorsed by ACC, AHA, HRS): “Each institution should have a written policy on IC [informed consent] that describes the process used to obtain consent, including timing, documentation, and surrogate decision-maker issues, as well as circumstances that would allow for exceptions to obtaining IC, such as emergency STEMI in a patient unable to provide consent.“
- 2021 ACC/AHA/SCAI revascularization guidelines: “In patients undergoing coronary angiography or revascularization, adequate information about benefits, risks, therapeutic consequences, and potential alternatives in the performance of percutaneous and surgical myocardial revascularization should be given, when feasible, with sufficient time for informed decision-making to improve clinical outcomes.”
This is not just limited to cardiology, this is an interdisciplinary consensus. Published documents from professional societies representing OB/GYN, Emergency Medicine, Neurology, Critical Care, Gastroenterology, General Surgery, Pediatrics, Anesthesiology, and I’m sure many others all consistently affirm the ethics of intervention in emergency situations where informed consent is impossible to obtain.
In addition to the above, the note actually says that both general cardiology and the critical care team felt intervention was indicated and proposed two physician consent. The interventional team wrote a procedure H&P that day (hospital day 3), but again did not take the patient for angiogram. The patient was extubated that afternoon.
On hospital day 4, the patient was neurologically intact and complaining of persistent chest pain. He underwent coronary angiography. The cath report describes subtotal occlusion of the mid left circumflex due to acute plaque rupture with TIMI II flow, as well as non-culprit lesions in the LAD and RCA. The patient had a stent placed in his LCx. Echocardiogram showed LVEF 50% with hypokinesis of the inferolateral wall.
Final diagnosis NSTEMI.
Smith: “NSTEMI” is a worthless diagnosis! It means nothing except that the EKG did not show ST Elevation. Absence of ST elevation has almost zero physiologic meaning and should have zero management consequences.
Discussion
Once again, we see that the standard for STEMI is almost impossible to attain. It is not enough to have transmural infarction of the lateral wall with acute occlusion of the LCx due to acute plaque rupture and persistently impaired coronary flow 4 days later. It is not enough for a patient to present with VF arrest during exertion and an ECG showing STEMI, interpreted as ** ** STEMI ** **.
No, this is described as “transient ST changes” in a patient with an ultimate diagnosis of NSTEMI. Who decides what is transient? There was no repeat ECG for 2 hours following the obvious STEMI, and even longer if you include the first ECG which was also diagnostic for OMI. With a long enough time horizon, every STEMI is transient! Instead, this label NSTEMI has nothing to do with any clinically important pathophysiology. Rather, it reflects the fact that intervention was delayed by physician choice. Summary of paper: it shows that the final diagnosis of STEMI vs. NSTEMI has nothing to do with either occlusion or ST Elevation, but only correlates with a door to balloon time less than, vs. greater than, 90 minutes.
In this case, one of the arguments put forth was inability to obtain consent, a circumstance that is both intuitively obvious to navigate and explicitly addressed in guideline statements in case any uncertainty remained.
Another consideration that sometimes arises is whether to intervene in a patient with unknown neurological prognosis, in this case a patient presenting with agonal respirations and fixed and dilated pupils. Immediately post arrest is not the time to make this judgment, and many such patients (like this one) have complete neurologic recovery. Unfortunately the same cannot be said for his infarcted myocytes.
= = =
==================================
MY Comment, by KEN GRAUER, MD (5/22/2026):
The frustration that we sometimes feel in our review of cases like the one presented today by Dr. Frick — is palpable in the title of this post = “STEMI: An Impossible Standard”.
- I find it hard to imagine any ECG “qualifying” for classification as a “STEMI” — if today’s 2nd ECG (done ~2 hours after the initial tracing) does not qualify.
- With this “theme” in mind — I focus My Comment on a few additional points to those put forth in Dr. Frick’s excellent discussion.
= = =
Today’s Initial ECG …
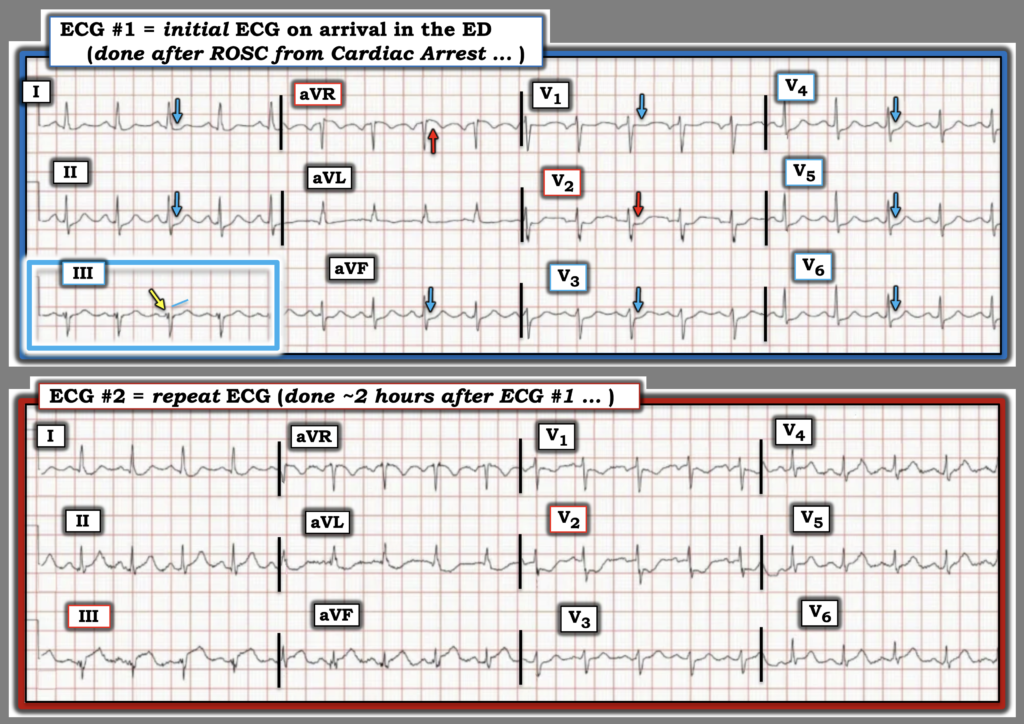
For clarity and ease of comparison in Figure-1 — I’ve put the first 2 ECGs recorded in today’s case together. Regarding the initial ECG (TOP tracing in Figure-1) — I considered 3 possible conclusions:
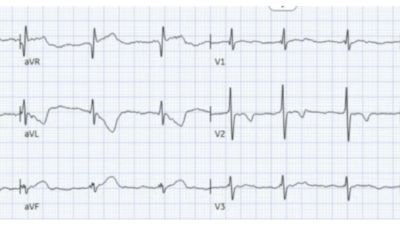
- Conclusion #1: In the context of significant sinus tachycardia — my “eye” was captured by the presence of diffuse ST depression that is present in at least 8/12 leads (9/12 leads if you count the clearly straightened ST segment in lead V1). In association with ST elevation in lead aVR — my initial impression was DSI (Diffuse Subendocardial Ischemia). As emphasized in My Comment in the July 25, 2024 post — DSI does not necessarily indicate acute coronary occlusion. And although many patients with DSI do have severe coronary disease — other conditions (ie, tachyarrhythmias, hypotension, anemia, etc.) may cause DSI in the absence of underlying coronary disease.
- Conclusion #2: Distinction between DSI vs acute posterior OMI is sometimes difficult. Posterior OMI is suggested when ST depression in the chest leads is maximal in lead V2 and/or V3 and/or V4 — whereas DSI is more likely when there is little distinction in the relative amount of chest lead ST depression and/or when ST depression is maximal in lateral chest leads V5 and/or V6. More than just the relative amount of ST depression — my “eye” was drawn to the shape of the shelf-like flattened and depressed ST segment in lead V2 (downward RED arrow in Figure-1) — so like Dr. Frick, I also strongly suspected acute posterior OMI in ECG #1.
- Conclusion #3: My 3rd “conclusion” turned out to be the one I favored most ==> both DSI and posterior OMI. In addition — I thought the straightened (but neither elevated nor depressed) ST segment takeoff in lead III of ECG #1 was different than the definite ST depression in the other 2 inferior leads (leads II,aVF) — such that ECG #1 manifested certain features of an Aslanger Pattern, in which the lead III ST-T wave appearance might be signaling ongoing inferior OMI in this patient with ECG signs of associated posterior OMI and DSI (See My Comment in the November 14, 2025 post — for another example of these Aslanger-like features).
- In support of my 3rd Conclusion — the fragmented initial component of the rS complex in lead III (YELLOW arrow) in my experience very often serves as a marker for a “pseudo-Q wave” that indicates inferior infarction has occurred at some point in time.
BOTTOM Line: Clinically — it does not matter which of my 3 Conclusions is the “correct” one — because IF the diffuse ST-T wave abnormalities seen in ECG #1 persist in this patient who has just been resuscitated from cardiac arrest — prompt cath will be indicated regardless — in order to define the anatomy (and perform PCI if there is evidence of coronary occlusion).
- P.S.: As cautioned by Dr Smith (also in the July 25, 2024 post) — When diffuse ST depression is seen in the initial ECG obtained following ROSC from cardiac arrest — It is usually best to repeat the ECG after waiting ~15 minutes — to see if the diffuse ST-T wave abnormalities are resolving (as they might if the ST depression was simply the result of transient “no flow” from the cardiac arrest— and not due to acute infarction).
= = =
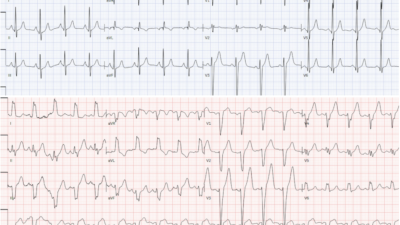
Figure-1: Comparison of the first 2 ECGs in today’s case.
= = =
Comparison of ECG #1 with the Repeat ECG …
As per Dr. Frick — the repeat ECG that I’ve reproduced in Figure-1 clearly establishes an acutely evolving infero–postero-lateral STEMI.
- Rather than waiting 15 minutes before repeating today’s initial ECG — 2 hours passed! This delay is unfortunate — as it may have contributed to the failure to perform prompt cath and PCI on today’s patient.
- Had the marked progression of ST-T wave abnormalities seen in ECG #2 been noted just 15 minutes after ECG #1 (instead of waiting 2 hours) — the need for prompt cath might have been compelling enough to convince providers to proceed with cardiac cath despite the patient’s persistent nonresponsiveness.
- ST elevation in all 3 inferior leads now clearly satisfies STEMI criteria (with obvious reciprocal ST depression in high-lateral leads I and aVL).
- The especially marked ST elevation in lead III of ECG #2 supports my earlier suspicion of an Aslanger-like pattern — with the learning point that the isoelectric ST segment straightening in lead III of ECG #1 in the context of ST depression in the other 2 inferior leads is potential indication of developing inferior OMI.
- The now clear ST depression and T wave inversion that we see in lead V1 of ECG #2, in association with now marked deepening and downsloping of the ST segment in neighboring lead V2 — is in support of my earlier suspicion from ECG #1 of posterior OMI from the subtle isoelectric flattened ST segment in lead V1 and the shape of the depressed ST segment in lead V2.
- Finally — the lateral chest lead ST depression in ECG #1 — has now been replaced by rising J-point ST elevation in these lateral chest leads, consistent with the LCx “culprit” found on cath.
= = =
Final Learning Points:
The “beauty” of retrospectively reviewing serial tracings by placing the ECGs you are comparing side-by-side (as seen in Figure-1) — is that after you take note of how the ECG evolved (as is seen in ECG #2) — You can then go BACK to the initial ECG and much better appreciate:
- i) That the subtle suggestion of an Aslanger-like Pattern within the BLUE rectangle in ECG #1, serves to distinguish the ST-T wave appearance in lead III from the different appearance ( = definite ST depression) that is seen in the other 2 inferior leads;
- ii) That the subtle isoelectric ST segment flattening in lead V1 of ECG #1 is not a normal finding — but instead is consistent with the evolving pattern of a posterior OMI that becomes much more obvious in ECG #2; — and,
- iii) That the different shape of the ST segment in lead V2 of ECG #1 showing shelf-like ST depression (RED arrow in lead V2) compared to upsloping ST depression in the 4 remaining chest leads — served as a sign of what might be forthcoming ( = the profound downsloping ST depression in lead V2 that developed in ECG #2).
- iv) And in retrospect — the reason the shape of the ST depression in leads V3,V4 of ECG #1 is upsloping (and not “shelf-like flat”, as it is in lead V2) — is that ST depression in these other chest leads is being attenuated by what was soon to become J-point ST elevation from the LCx “culprit” that becomes evident in ECG #2.
= = =
=