==================================
Case Presentation by KEN GRAUER, MD (5/5/2023):
— Edits by Drs. Meyers & Smith …
==================================
Dr. Smith was reading ECGs — and he sent myself and Dr. Meyers the tracing shown in Figure-1. At the time we did not yet know the history …
- What do YOU think?
 |
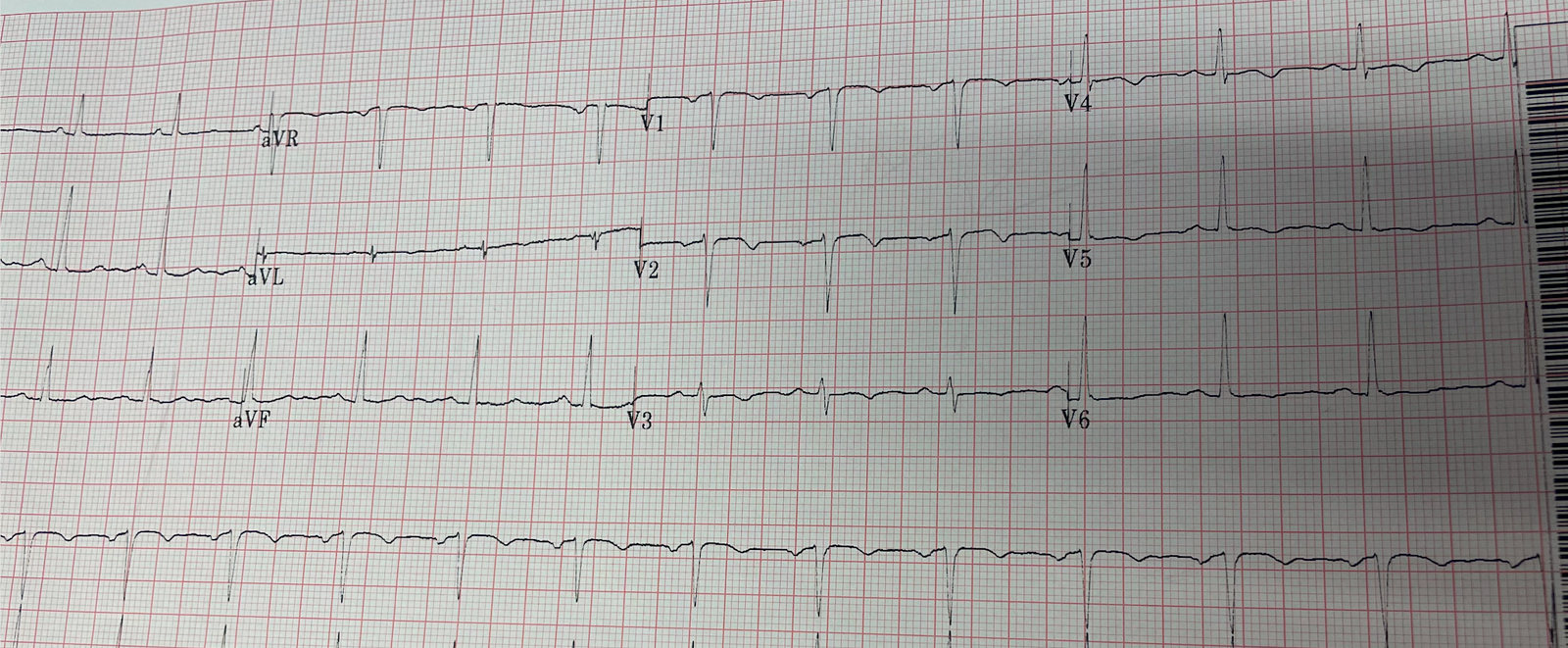
| Figure-1: The initial ECG in today’s case. No history yet … |
Our Initial Thoughts on the ECG in Figure-1:
- Dr. Meyers said the following: “I see 2 different atrial foci — one sinus and one ectopic. There is AV block — but unclear why. T waves in leads V4-thru-V6 appear peaked — so possible hyperkalemia.”
- My Thoughts: I was struck by the unusual shape of deflections that I labeled a, b, d, e, and h — and by the fact that despite the high amplitude of deflection b in leads II and III, there was no deflection at all corresponding to b in lead I (See Figure-2). In addition — the amplitude of deflection d in leads aVR and aVL was approximately 1/2 the amplitude of d in lead aVF. These mathematical relationships of relative deflection size with absence of any deflection at all in lead I — are most commonly encountered when there is some type of artifact caused by movement or other interference originating from the Left Leg.
- I thought the lack of any QRS complex after deflections b, e and h supported my theory of some kind of artifact distortion.
- Regarding the rest of the 12-lead tracing in Figure-1 — there was increased R wave amplitude in the lateral chest leads — and anterior T wave inversion (not surprising given the overly slow ventricular rate) — but not suggestive of an acute cardiac event.
QUESTION:
- Do YOU agree with either Dr. Meyers or myself?
 |
| Figure-2: I’ve labeled by letter the deflections in the long lead II. |
The CASE Continues:
A little while later — a 2nd ECG was done. We still did not know any history …
- Does this repeat ECG seen in Figure-3 provide some answers?
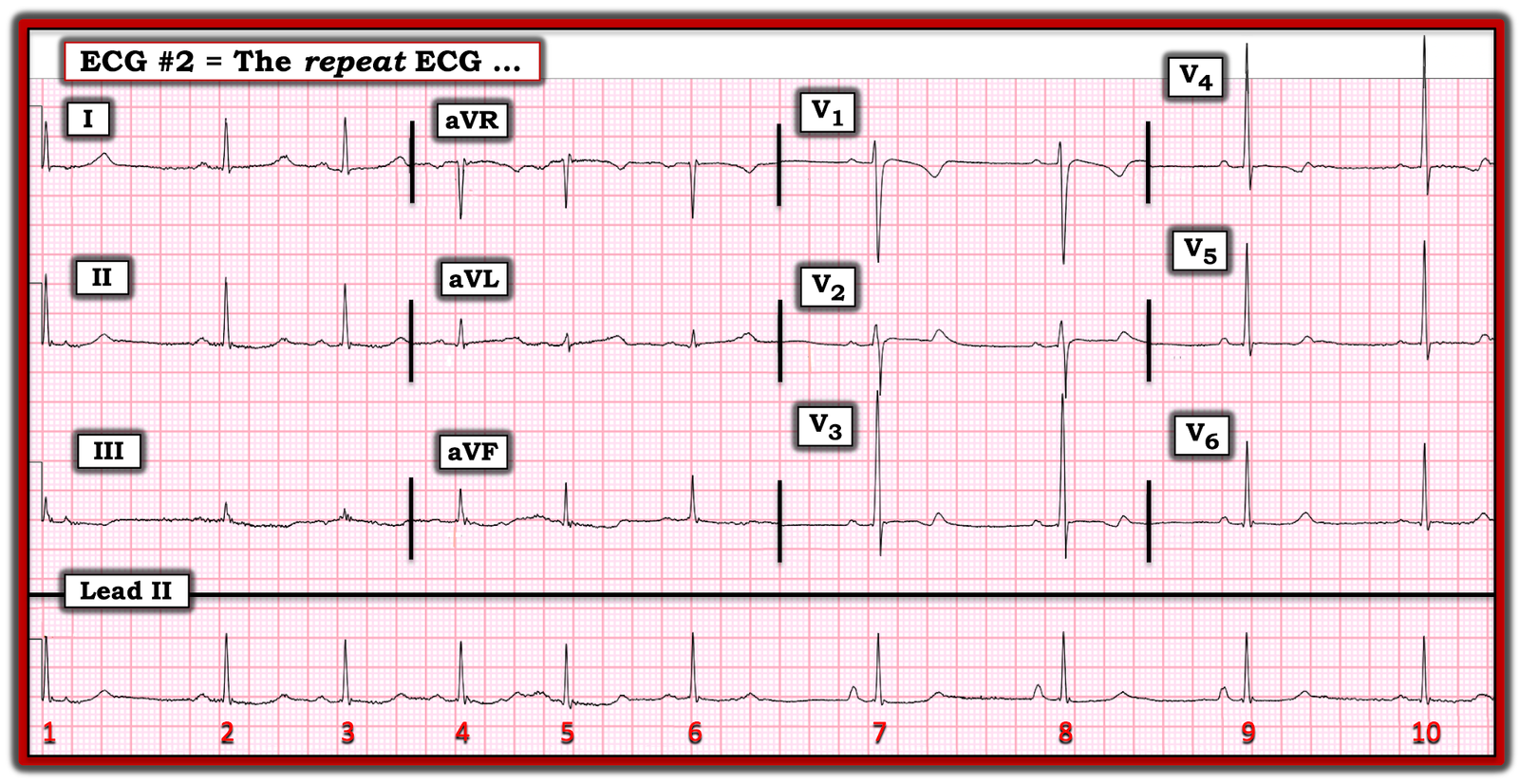 |
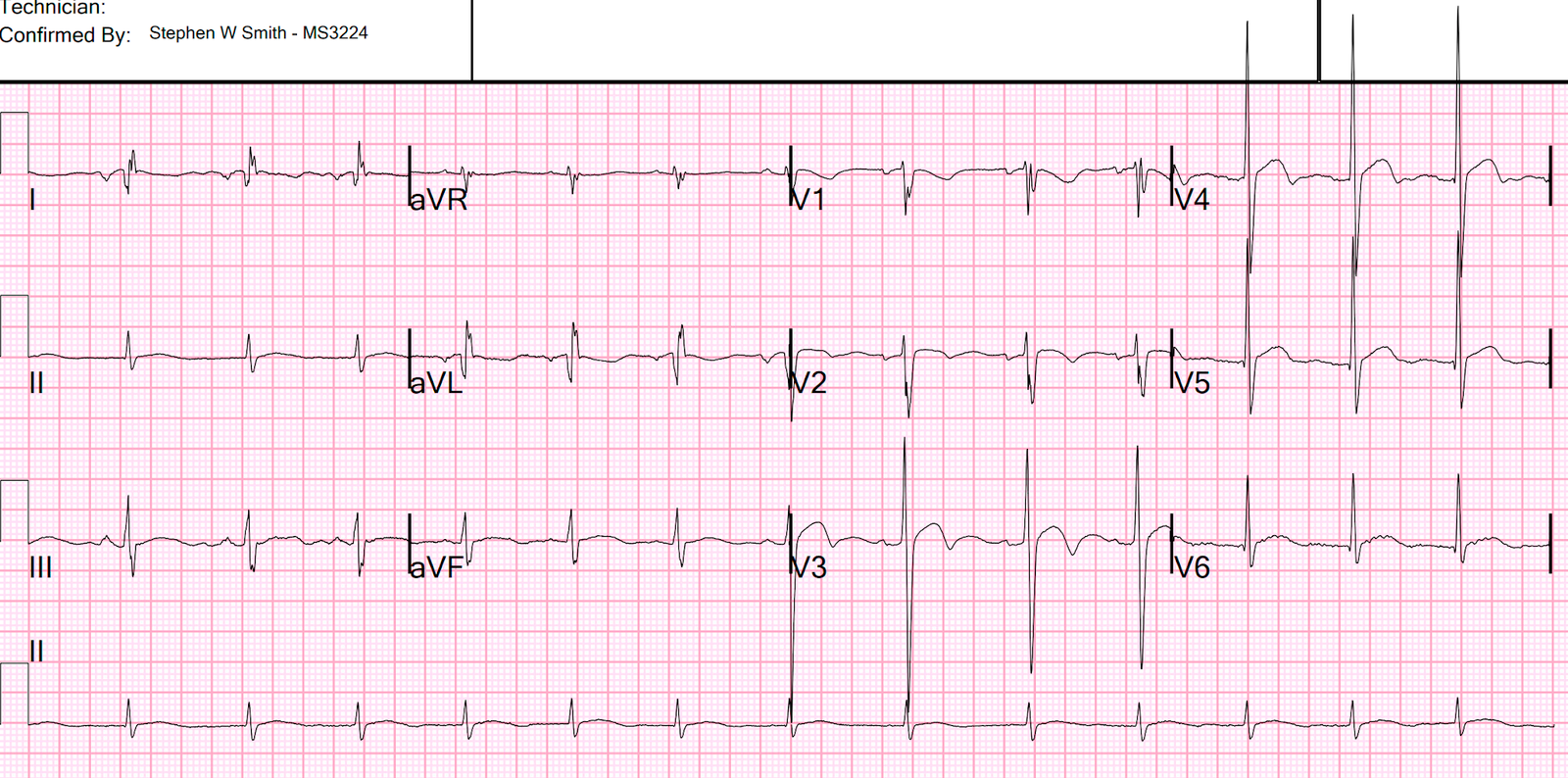
| Figure-3: The repeat ECG in today’s case. |
Our Thoughts After Seeing the ECG in Figure-3:
Immediately on seeing ECG #2 — Drs. Meyers, Smith and myself knew that my theory about artifact was not correct …
- Each QRS complex in the long lead II rhythm strip in Figure-3 is now clearly preceded by a conducting P wave.
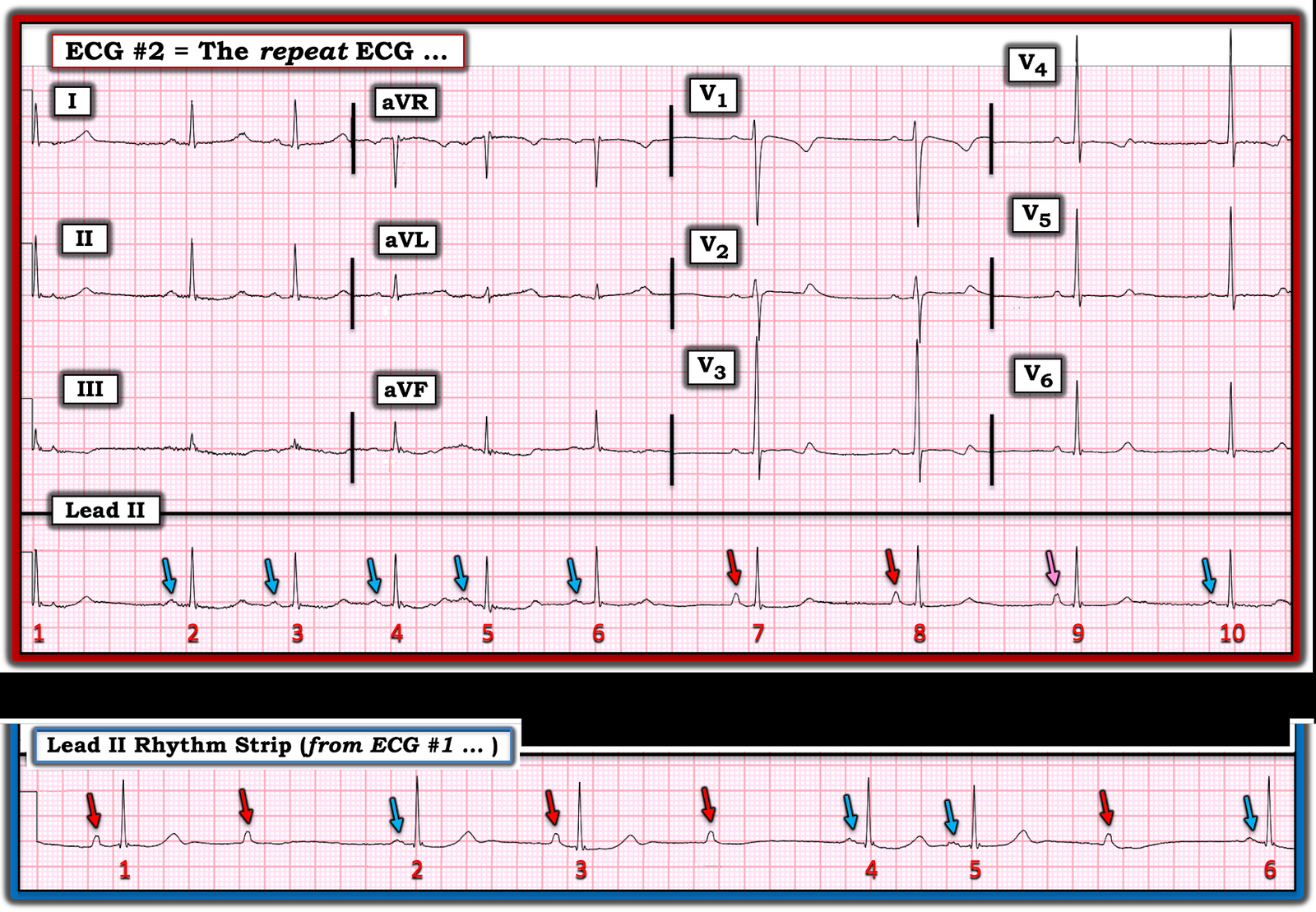
Putting It All Together:
For clarity in Figure-4 — I’ve labeled with colored arrows all P waves in the long lead II rhythm strips from the 2 ECGs done in today’s case.
- There are 2 atrial foci — which I represent with RED and BLUE arrows. I suspect that the deflections that I initially thought represented artifact (ie, the RED arrows) are sinus P waves — and that the BLUE arrows represent an atrial escape focus.
- Looking first at the long lead II rhythm strip in ECG #2 — the rhythm begins with 5 beats conducted by the escape focus (ie, beats #2-thru-6). The R-R interval from this escape focus begins to slow with beat #6 — after which the escape focus pauses …
- The sinus node “wakes up” with beat #7. Note that the PR interval preceding beats #7 and 8 is the same — proving these deflections are conducting.
- Beat #10 is once again conducted by the escape focus.
- The P wave preceding beat #9 is not quite as tall as the P waves preceding beats #7 and 8. I labeled this P wave with a PINK arrow in Figure-4 — as I believe it represents an atrial fusion beat that occurs during transition from sinus P waves to the escape atrial focus that takes over again with beat #10.
Armed with the knowledge that all colored arrows represent P waves — events in the long lead II rhythm strip from ECG #1 now make much more sense:
- The long lead II from ECG #1 begins with a sinus beat — but the 2nd sinus P wave ( = the 2nd RED arrow in the bottom rhythm strip) is not conducted! This results in a pause of 2.35 seconds — until finally, the atrial escape focus comes to the rescue (BLUE arrow in front of beat #2).
- Beat #3 is sinus conducted — but it is followed by another non-conducted sinus P waves ( = the 4th RED arrow). There follows 2 atrial escape beats (#4 and #5) — another non-conducted sinus P wave — and finishes with escape beat #6.
What Does this All Mean?
At this point — I still did not know the history in this case. My thoughts were the following:
- ECGs #1 and #2 showed a completely unreliable sinus pacemaker, with presumed high-grade 2nd-degree AV block — and frequent resultant pauses of over 2 seconds (that would have been even longer had it not been for intermittent relief from the atrial escape focus).
- KEY to management will be finding a hopefully treatable cause of this unusual bradycardic rhythm disturbance. Common explanations for unusual rhythms such as this one include: i) Hyperkalemia (or other severe electrolyte disorder); ii) Recent infarction/ischemia; iii) Sleep apnea; iv) Severe hypothyroidism; v) Acute neurologic catastrophe (ie, stroke, bleed, trauma, tumor); vi) Some other toxicity.
- IF none of the above explanations are operative — then especially if the patient is older, the diagnosis will almost certainly be SSS ( = Sick Sinus Syndrome), and permanent pacing will be needed.
CASE Follow-Up:
We finally found out the history in today’s case! The patient was a 20-something woman who was found poorly responsive with altered mental status in her car. Numerous needles from self-injection of opioids were found in the car. Narcan was not given at the scene. There was no indication of hyperkalemia.
- Krantz et al authored a State-of-the-Art Review on Cardiovascular Complications of Opioid Use (JACC 77(2):205-223, 2021) — in which mechanisms from Opioid Overdose that detail arrhythmia production (up to cardiac arrest) are elucidated — thereby providing an explanation for the unusual arrhythmias in today’s case.
- The “good” news — Treatment with naloxone will probably resolve the bradycardia.
 |
| Figure-4: Review of the 2 long lead rhythm strips from today’s case. |
![]()