Written by Pendell Meyers
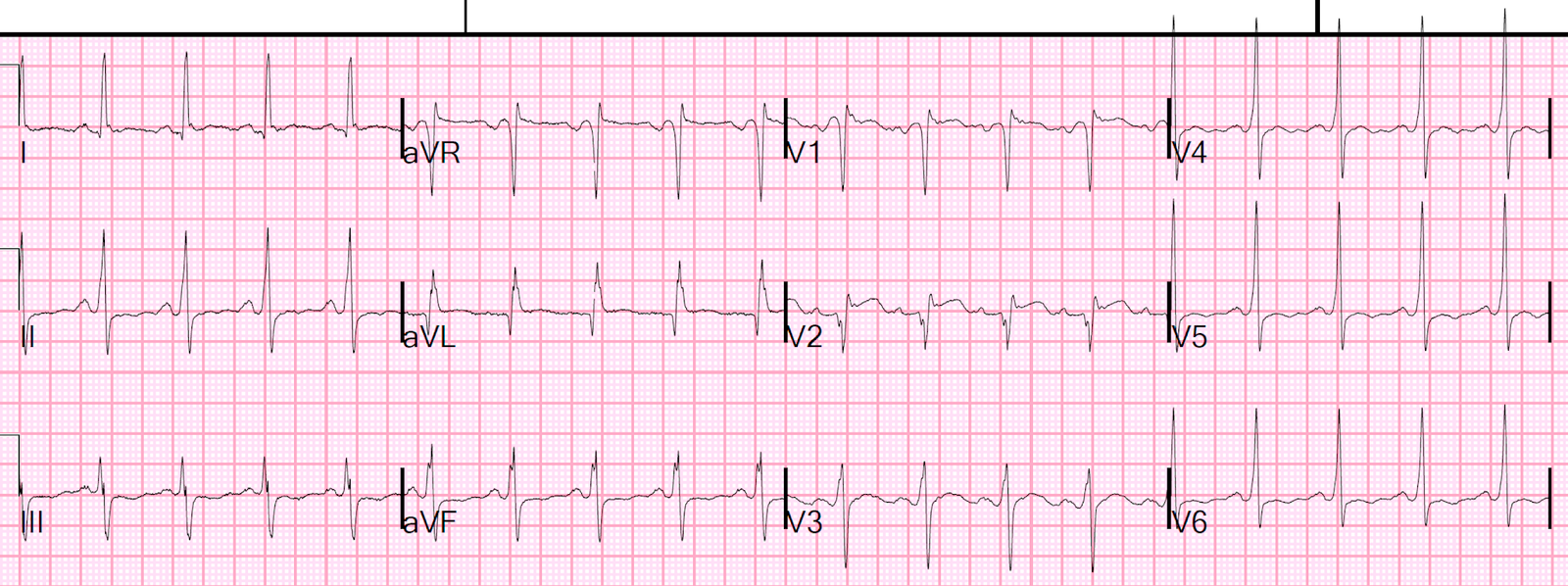
Let’s see this presentation ECG without any context first (no baseline ECG was available)
 |
| What do you think? What will you do? |
The ECG is diagnostic of severe hyperkalemia. There is sinus tachycardia, the beginning of QRS widening, tall pointy peaked T waves with little area compared to their height. There is STE in V1-V3, aVR, and aVL, with STD in II, III, aVF, V4-V6. The appearance in V1 is similar to the Brugada morphology (as is often the case in hyperkalemia and Na channel blocker effects causing STE). Together these ST elevations in the right precordial leads and aVL are classic pseudoSTEMI (or pseudoOMI) patterns seen in hyperkalemia (see the end of the post for links to many similar cases). This ECG shows no evidence of OMI despite the fact that it meets STEMI criteria – it is all hyperK. Of course there may also be an additional component of acidosis, peri-ROSC, etc, given the context below, but hyperkalemia is the most contributory factor.
This was a man in his 30s who was found down and altered. He was seen normal the day before, then found in his bed by a friend, unresponsive. CPR was administered. EMS arrived and found him in PEA arrest. He was given epinephrine, calcium, and bicarbonate, and after several rounds of CPR he was found to have a pulse. He was intubated in the field. He was tachycardic and hypotensive. EMS recorded this ECG above just before arriving to the ED.
When the ED provider saw this ECG, they activated the cath lab thinking it was “STEMI” (presumably, this means that they thought the ECG meant that the patient was suffering from an acute coronary occlusion). Although it is irrelevant, this ECG does have acute STE that meets STEMI criteria in V1 and V2.
Cardiology reviewed the ECG remotely and heard the initial history, and decided that they did not want to take the patient to the cath lab.
The initial potassium returned at 7.9 mEq/L.
At this point, further history and physical exam was performed, and it was realized that the patient was suffering from severe rhabdomyolysis and lower extremity compartment syndrome from prolonged down time, presumably due to drug ingestion.
Calcium was given IV, as well as insulin. I am not sure what dose or type of calcium.
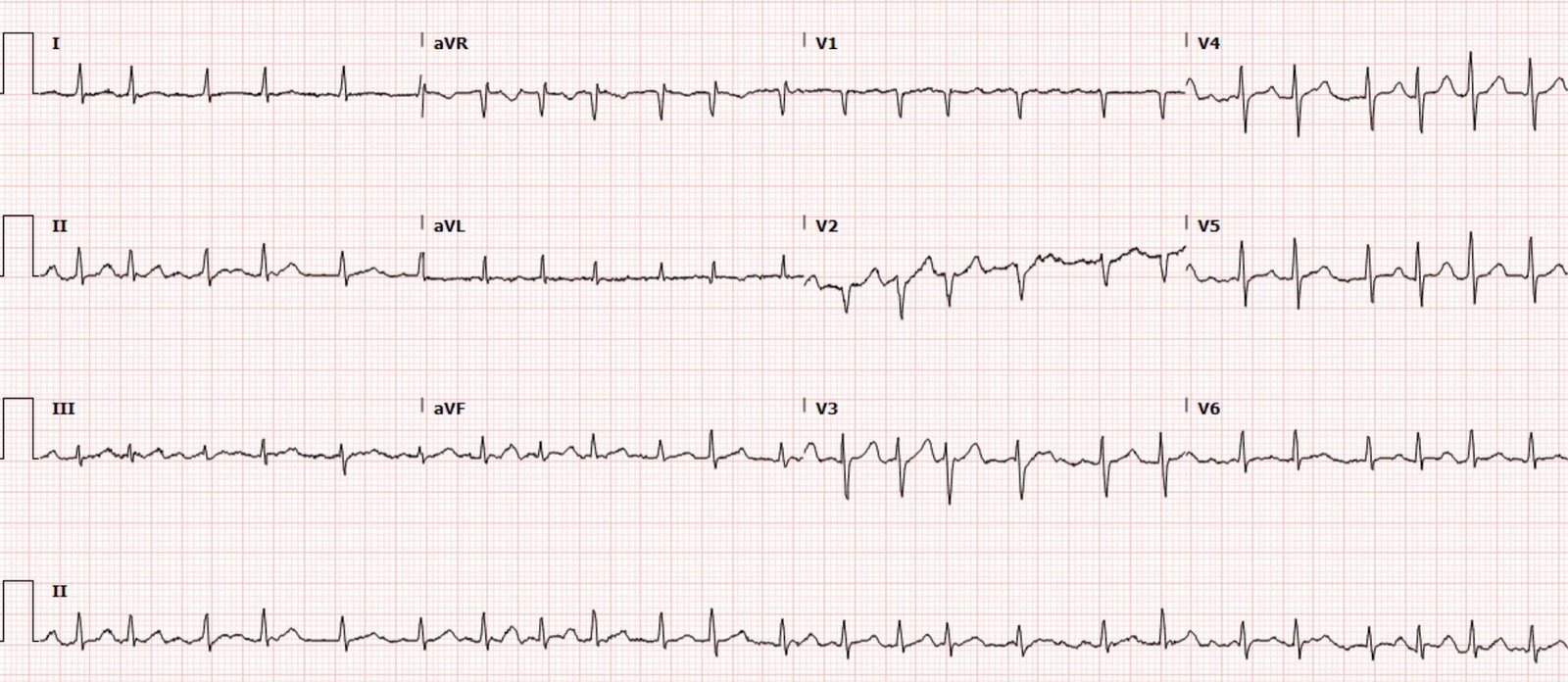
Within minutes of calcium administration, a repeat ECG was recorded:
 |
| Findings almost completely resolved. |
The patient unfortunately suffered a long and rocky ICU course.
Learning Points:
Hyperkalemia is one of the most important diagnoses that can be made using the ECG. We must memorize these hyperkalemia ECG patterns to recognize them immediately in practice. Failure to do so may lead to early diagnostic closure (like in his case), which may result in delayed care, unnecessary procedures, and patient harm!
When hyperkalemia causes STEMI mimics, in my experience the most common areas for the STE are in the right precordial leads (V1-V2), lead aVL, and the inferior leads.
ECGs are almost always better when interpreted with the clinical context, but some ECGs are diagnostic by themselves in confusing scenarios.
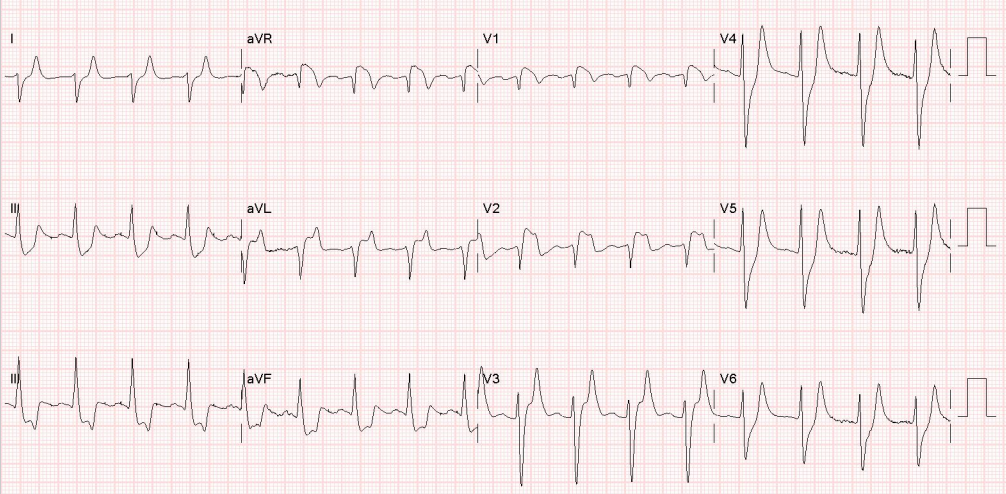
Here are more examples of hyperkalemia OMI and STEMI mimics: