A 50-something male with h/o CAD and CABG, and dual chamber pacemaker due to sick sinus syndrome, called 911 for onset of acute chest pain 2 hours prior.
Here was the prehospital ECG:
 |
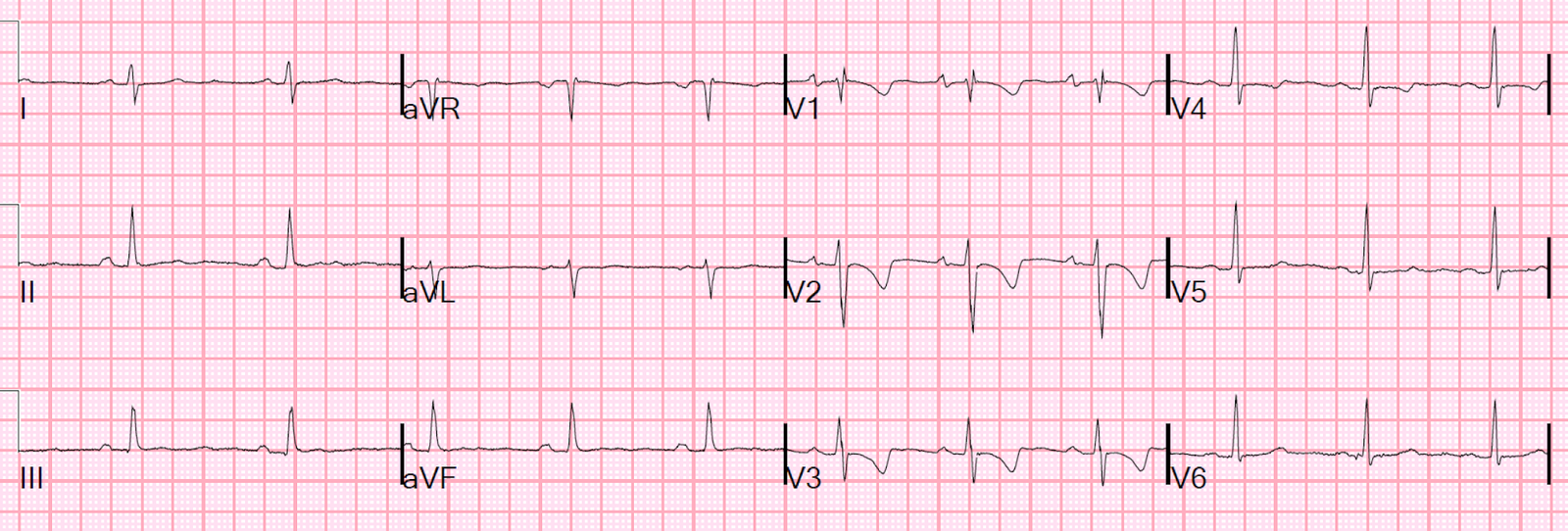
| There is sinus rhythm with very long PR interval (about 300 ms).
There is a wide QRS [(nonspecific intraventricular conduction delay (IVCD)] Neither RBBB nor LBBB There is some ST elevation discordant to deep wide S-waves in III and aVF, and V3 and V4, appears baseline. There is some reciprocal ST depression in aVL, but this is normal when there is ST elevation in III that is likely to be due to LBBB, LVH, IVCD, or WPW (in this case, it appears to be due to IVCD) V1 has some ST elevation, and V2 has absence of expected discordant ST elevation, with a very flat ST segment. This is all non-diagnostic. |
The medics brought the patient to the critical care area, as they were suspicious of acute MI.
The pain started at rest, was constant, sharp in the sternum and radiating to the jaw and left arm and into the upper back, associated with diaphoresis but no SOB. No history of venous thromboembolism. It was not relieved with nitroglycerin at home, but decreases from 9/10 to 7/10 after EMS gave NTG. He stated it felt like a prior MI.
Here is the first ED ECG, at time zero:
 |
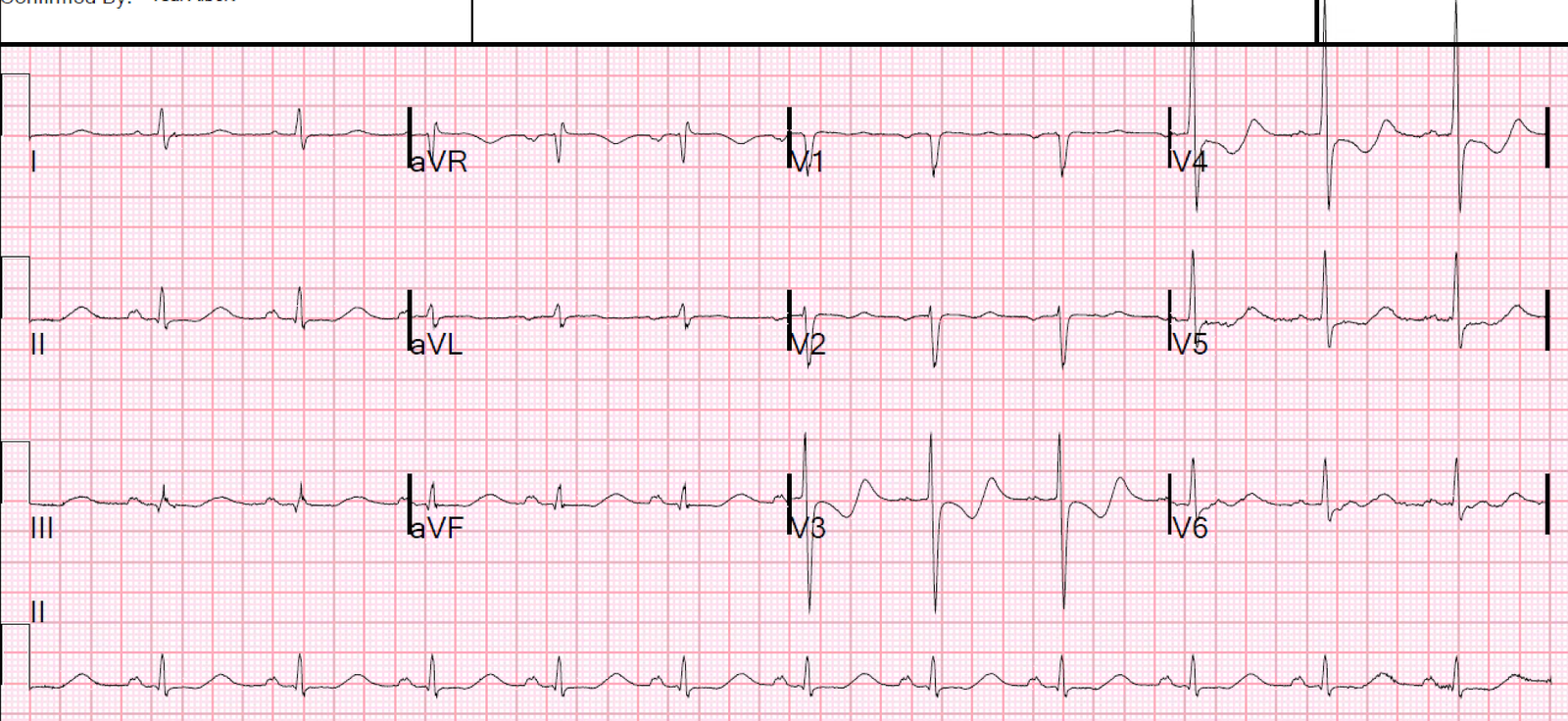
| There is a wandering baseline in the limb leads. Nevertheless, there is a suggestion of proportionally excessively discordant ST elevation in inferior leads, with proportionally excessively discordant reciprocal ST depression in aVL. There is also almost excessively discordant ST elevation in precordial leads, but due to wandering baseline, it is hard to say whether it reaches 25% of the preceding S-wave. Lots of change since the prehospital ECG! |
The prehospital ECG has normal conduction without ischemic ST elevation.
The ED ECG now has a ventricular paced rhythm (VPR).
The ED ECG now has new ST Elevation.
Is all this new ST elevation only due to VPR.
No!
Smith modified Sgarbossa criteria (for use in LBBB and in VPR):
Rule 1 (80-90% sensitive, 95% specific)
Any one of:
1. 1 mm concordant STE in any one lead.
2. 1 mm concordant STD in any one of leads V1-V3
3. At least 1 mm discordant STE that is greater than or equal to 25% of preceding S-wave in at least one lead.
Rule 2 (Only 64% sensitive, but 98% specific, for occlusion):
Any single lead with proportionally excessively discordant STE or STD of at least 30% of preceding S- or R-wave.
Lead aVL seems to have STD that is at least 30% of preceding R-wave.
Smith modified Sgarbossa criteria are being studied now in the PERFECT study (Paced ECG Requiring Fast Emergent Coronary Therapy). Preliminary Results are encouraging that they work in ventricular paced rhythm as well (not surprisingly). See abstract and references below.
___________________
Case continued
The physicians were worried about this, and 16 minutes later recorded this ECG:
 |
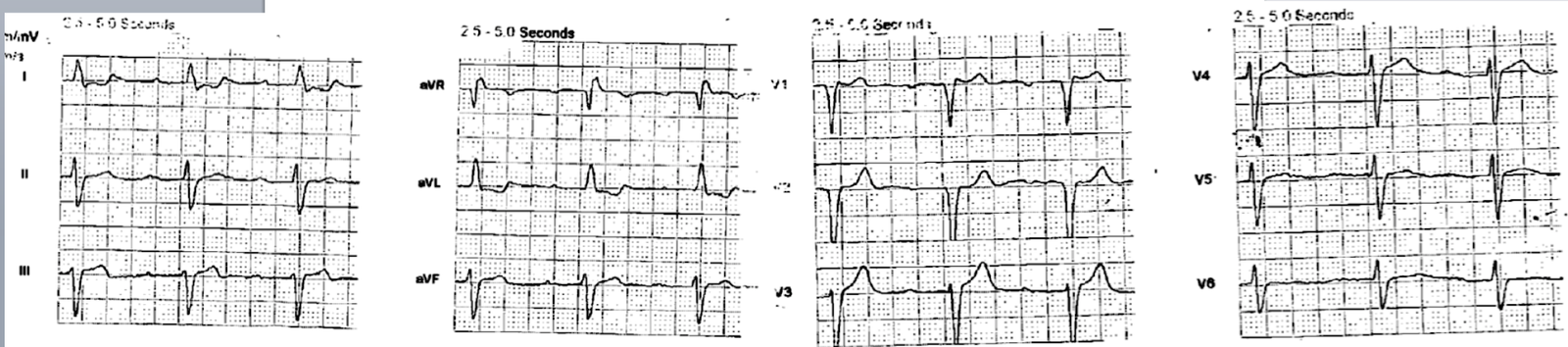
| Now there is clearly excessively discordant STE in III and aVF, with excessive STD in aVL. Notice there is also quite a bit of ST elevation in V1; is this due to RV MI? |
The cath lab was activated.
It was a very interesting angiogram.
There was a known chronically occluded proximal RCA, proximal to the RV marginal branch supplying the RV.
The RCA distal to this was known to be supplied by a CABG graft to the posterolateral branch of the RCA (on the posterior wall!), such that flow to the RCA was retrograde.
This posterolateral branch (not the graft itself) was occluded such that that branch could no longer supply the inferior wall and the RV.
Therefore, it caused inferior and RV STEMI.
It was opened and stented with good results.
Full angiogram report:
1. Left main: patent stent.
2. LAD: 70% stenosis in the mid segment at the take-off of a diminutive D1 (angiographically unchanged from previous angiography in 9/2017), then >90% stenosis after D2 (D2 has a 2.0-2.5 mm caliber). The distal LAD is supplied by a patent LIMA.
3. LCX: chronically occluded. The OM is supplied by a patent vein graft.
4. RCA: known chronic occlusion, therefore not studied. The RPLA is supplied by a patent vein graft. Antegrade flow into the RPLA is good, however, retrogradely the RPLA is occluded with contrast hang-up indicative of a thrombotic occlusion. Hence the flow to the RPDA is compromised.
Here is the post intervention ECG:
 |
| Atrial, but not ventricular, pacing.
STE resolved T-wave inversion (reperfusion T-waves) in inferior leads. Reciprocally upright T-wave in aVL Lateral T-wave inversion. Was there indeed ischemia in the myocardial territory under V3-V6? |
The patient went into a paced rhythm, and so had a paced ECG recorded about the same time post cath as the above ECG:
 |
| Post cath with some ventricular paced beats and some native beats with atrial pacing.
V1-V3 and the first complexes of V4-V6 have ventricular paced beats. In the paced beats: There is new STE in V2 with a large upright T-wave, suggesting that the first paced ECG, with isoelectric ST segment in V2, was due to posterior MI. There is less STE in V3-V6, and some T-wave inversion, suggesting that there was ischemia in this territory as well, that is now resolved. I’m not sure exactly how to correlate the angiogram with the findings in V3-V6. |
Peak troponin = 8.2 ng/mL
Echo:
The estimated left ventricular ejection fraction is 50 %.
Regional wall motion abnormality-basal inferior, hypokinetic.
Learning Point:
Modified Sgarbossa Criteria are very useful in Ventricular Paced Rhythm
Smith modified Sgarbossa criteria:
–>