Written by Pendell Meyers
A woman in her 40s presented with acute chest pain and shortness of breath. Vitals were within normal limits.
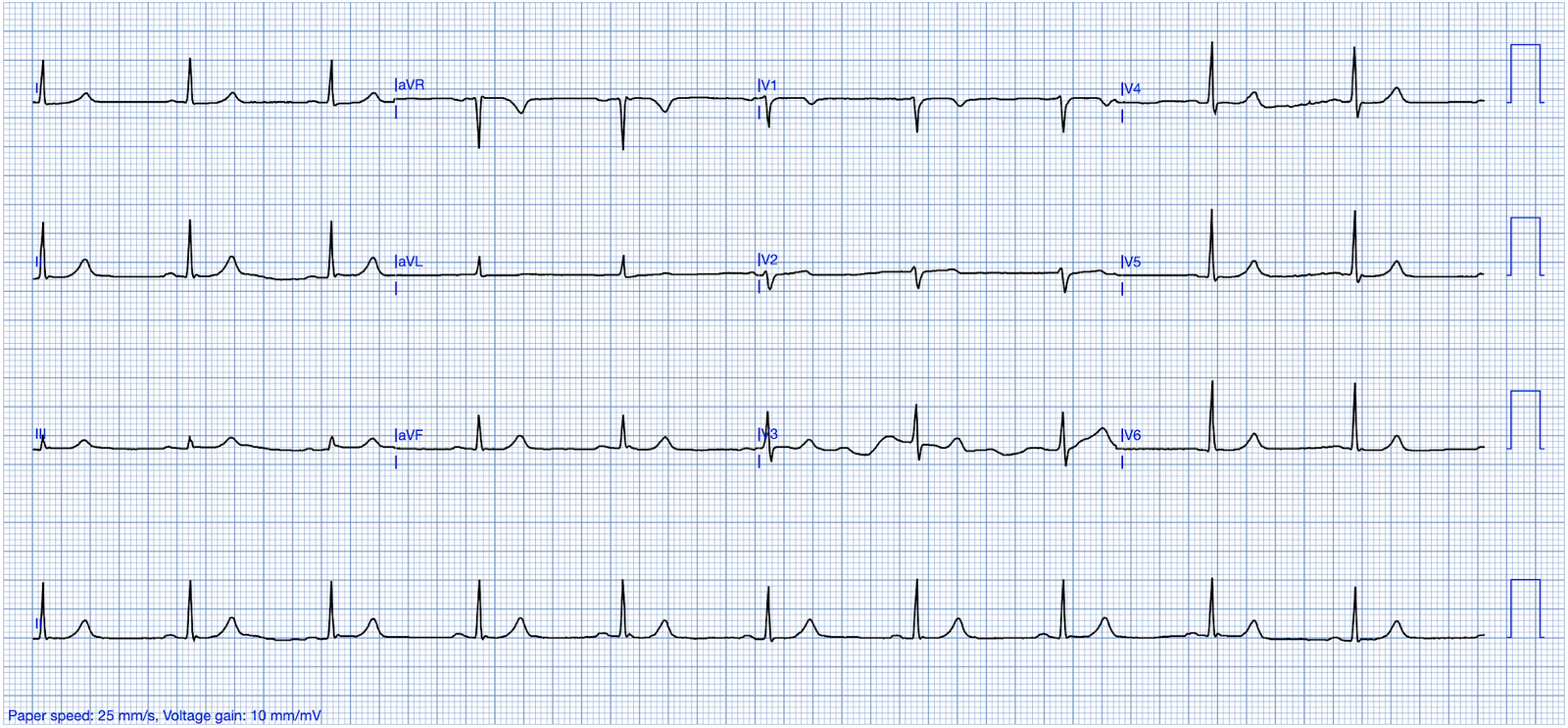
Here is her triage ECG:

— What do you think? —
= = =
Smith: This is classic for pulmonary embolism (PE). There are 2 key points to making this diagnosis on the ECG:
- 1) There is T-wave inversion which you might think is due to Wellens’ waves, but the patient has active symptoms, so it is not Wellens’ sydrome
- 2) The T-wave inversion in V1-V4 is accompanied by T-wave inversion in lead III. This is very specific for PE vs. ACS.
Also, and much less teachable: the T-waves just don’t look right for ACS.
= = =
Check out this post for an explanation of the T-wave morphology:
= = =
The Case Continues:
Acute right heart strain was suspected on ECG and bedside echo.
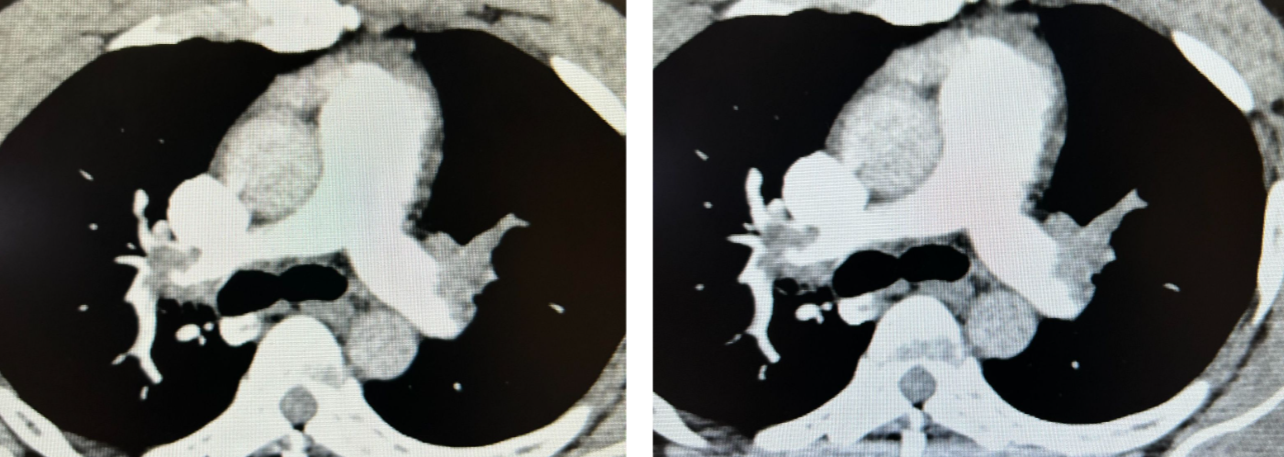
- Acute pulmonary embolism was confirmed on CT angiogram:
Follow-Up: The patient did well.
See our other acute right heart strain / pulmonary embolism cases:
- A man in his 50s with shortness of breath
- Another deadly triage ECG missed, and the waiting patient leaves before being seen. What is this nearly pathognomonic ECG?
- A man in his 40s with RUQ abdominal pain
- A woman in her 50s with shortness of breath
- When the ECG is more revealing than the HPI
- A crashing patient with an abnormal ECG that you must recognize
- A man in his 40s with a highly specific ECG
- Chest pain, ST Elevation, and tachycardia in a 40-something woman
- Repost: Syncope, Shock, AV block, RBBB, Large RV, “Anterior” ST Elevation in V1-V3
- A young woman with altered mental status and hypotension
- An elderly woman transferred to you for chest pain, shortness of breath, and positive troponin – does she need the cath lab now?
- A 30-something woman with chest pain and h/o pulmonary hypertension due to chronic pulmonary emboli
- A 30-something with 8 hours of chest pain and an elevated troponin
- Syncope, Shock, AV block, Large RV, “Anterior” ST Elevation….
- Dyspnea, Chest pain, Tachypneic, Ill appearing: Bedside Cardiac Echo gives the Diagnosis
- 31 Year Old Male with RUQ Pain and a History of Pericarditis. Submitted by a Med Student, with Great Commentary on Bias!
- Chest pain, SOB, Precordial T-wave inversions, and positive troponin. What is the Diagnosis?
- Cardiac Ultrasound may be a surprisingly easy way to help make the diagnosis
- Answer: pulmonary embolism. Now another, with ultrasound….
- This is a quiz. The ECG is nearly pathognomonic. Answer at bottom.
- Chest Pain, SOB, anterior T-wave inversion, positive troponinAnterior T wave inversion due to Pulmonary Embolism
- Collapse, pulse present, ECG shows inferior OMI. Then there is loss of pulses with continued narrow complex on the monitor (“PEA arrest”)
- What do you suspect from this ECG in this 40-something with SOB and Chest pain?
= = =
======================================
MY Comment, by KEN GRAUER, MD 11/21/2024 — Updated for WordPress on 2/24/2026):
Today’s case by Dr. Meyers serves as one more reminder of an entity that we need not to miss = Acute PE (Pulmonary Embolism).
- At the end of Dr. Meyers’ discussion — he lists more than 20 links to cases that we’ve presented related to this entity on Dr. Smith’s ECG Blog. That said — the diagnosis of acute PE continues to be overlooked (and the ECGs of such patients continue to be misinterpreted as acute ischemia or infarction — instead of being recognized as diagnostic of acute PE).
= = =
The ECG Diagnosis of Acute PE:
We’ve reviewed the ECG clues to acute PE in those more than 20 links that Dr. Meyers’ lists above. I found today’s initial ECG interesting — in that most of the time, the ECG diagnosis of acute PE is highlighted by more than just a couple of the ECG Findings that I list below in Figure-2.
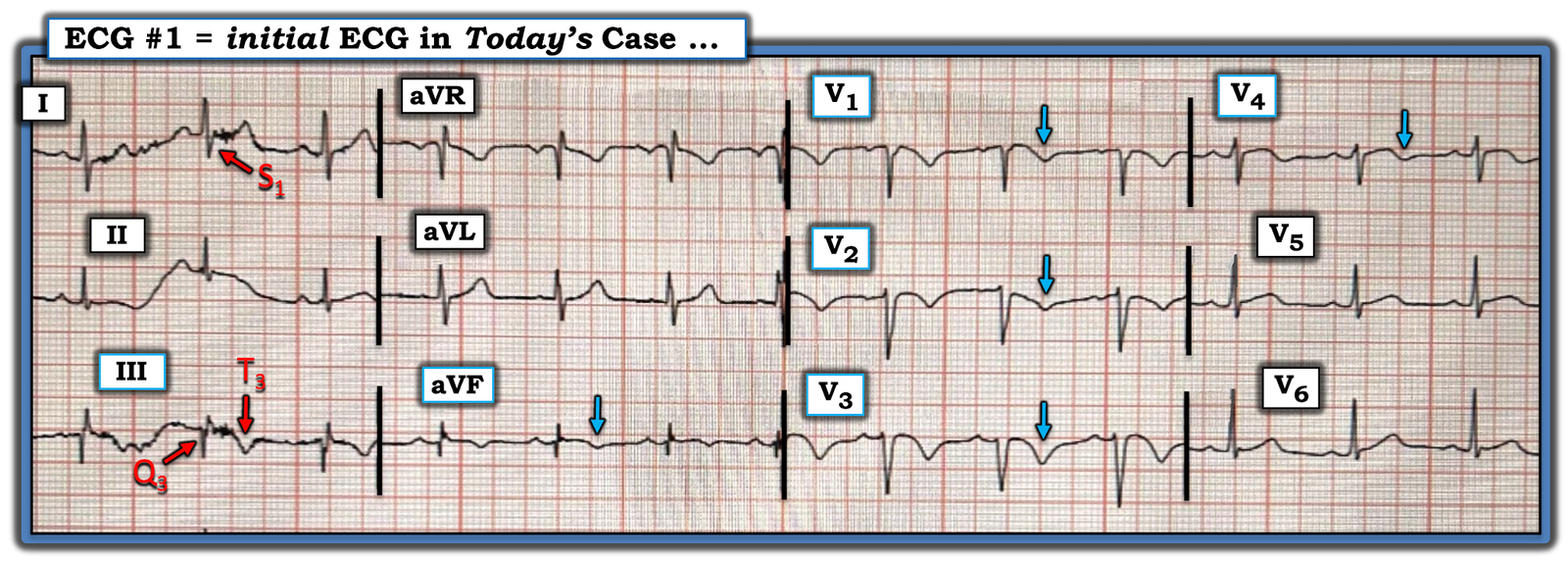
- For example, in today’s initial ECG (that I’ve reproduced and labeled in Figure-1) — there is no sinus tachycardia — and no right axis, RAA, incomplete or complete RBBB, tall R in lead V1, persistent precordial S waves, ST elevation in lead aVR or AFib.
That said — the following are present in today’s case:
- A suggestive History (shortness of breath with chest pain as the chief complaint).
- An S1Q3T3.
- Deep symmetric T wave inversion in the anterior chest leads (BLUE arrows in Figure-1) — that occurs in association with T wave inversion suggesting RV “strain” is present not only in the anterior chest leads, but also in inferior leads III and aVF.
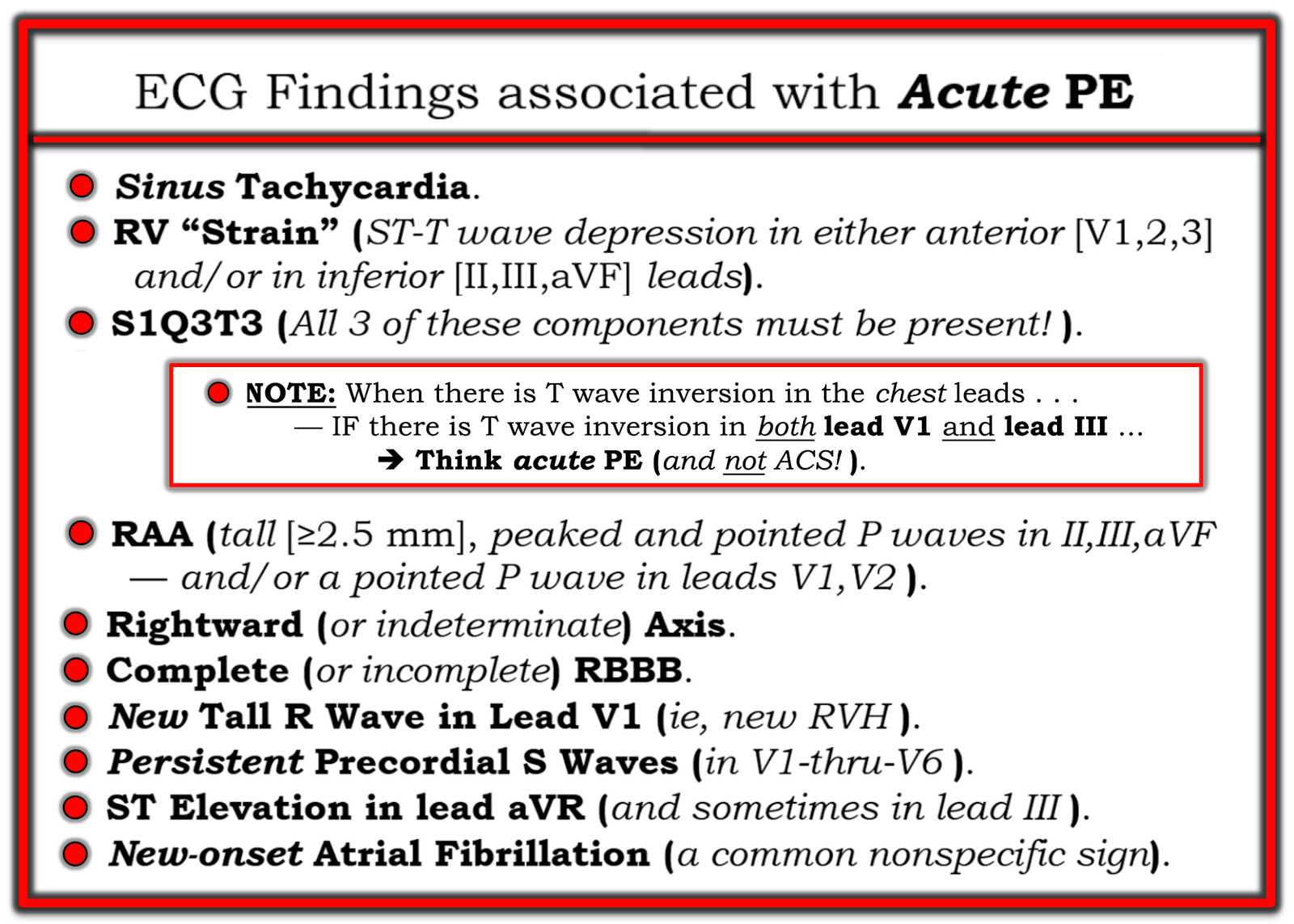
PEARL (as per Drs. Meyers and Smith): When there is T wave inversion in the chest leads — IF there is T wave inversion in both lead V1 and lead III ==> Think acute PE (and not ACS! ).
- By itself — the S1Q3T3 sign seen in Figure-1 would not be specific for acute PE (ie, I have seen this sign in healthy individuals with no acute pulmonary pathology). However, in the presence of a suggestive history and the extensive T wave inversion seen in today’s case — the S1Q3T3 strongly supports the diagnosis of acute PE.
- T wave inversion as diffuse as is seen in Figure-1 — most often suggests a sizeable PE (which makes it all the more surprising that there is no tachycardia and a lack of more of those ECG findings that are listed in Figure-2).
- Finally — the Q in lead III — the ST coving with slight ST elevation + T wave inversion in leads III and aVF — and the ST segment straightening in lead aVL — might lead one to misinterpret today’s ECG as indicative of ACS. IF tempted to do so — it is worth rereading the above PEARL!
- CT angiogram confirmed the diagnosis of acute PE.
= = =
Figure-1: I’ve labeled the initial ECG in today’s case.
= = =
Figure-2: ECG Findings associated with acute PE.
= = =
= = =
= = =