A prehospital cath lab activation for STEMI came through with the information that the 40-something woman had chest pain and a pulse of 140.
We were immediately skeptical that the patient had a STEMI because of the high heart rate. She would have to be in cardiogenic shock with a massive STEMI for that. Certainly possible, but when the heart rate is so high, be skeptical.
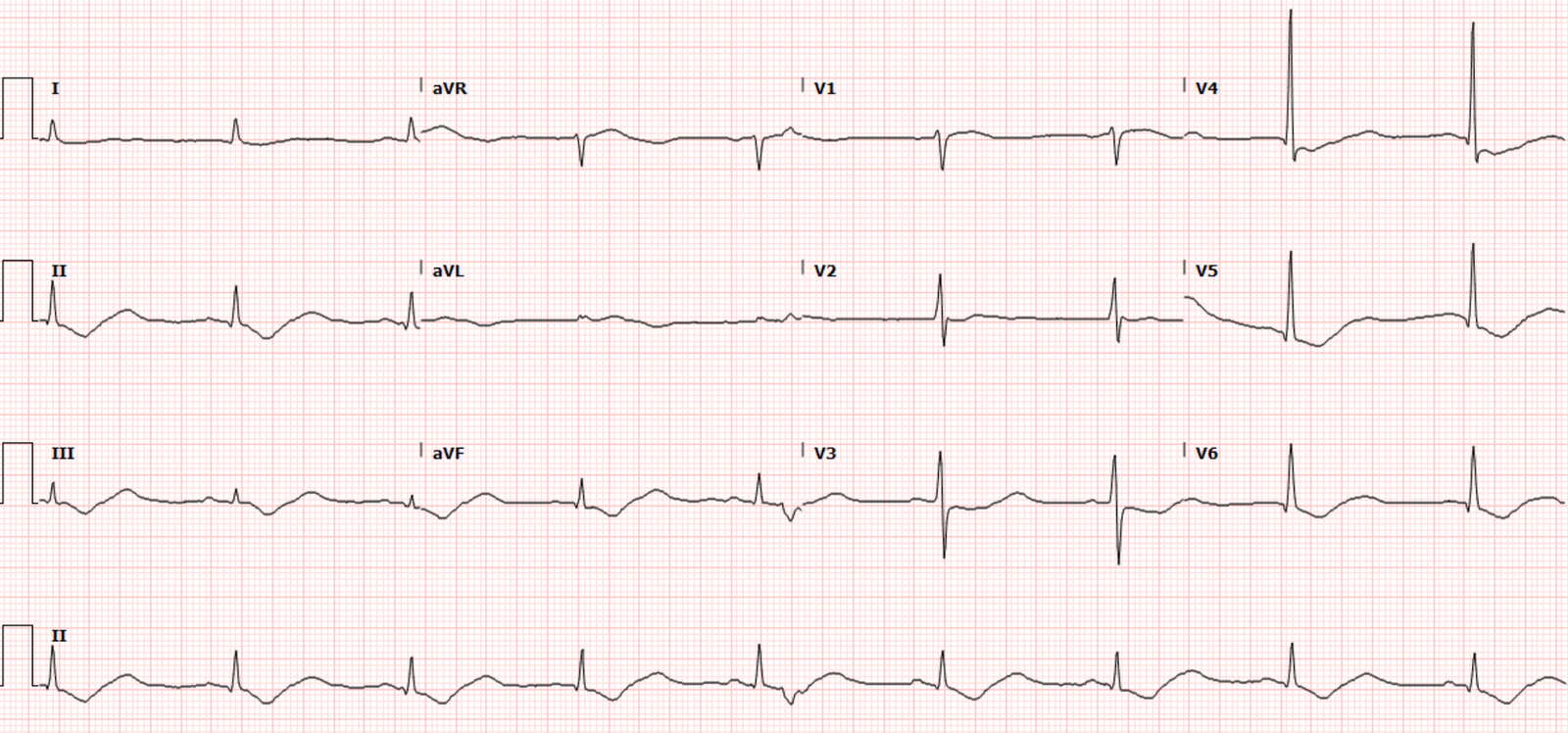
The patient arrived with this ECG:
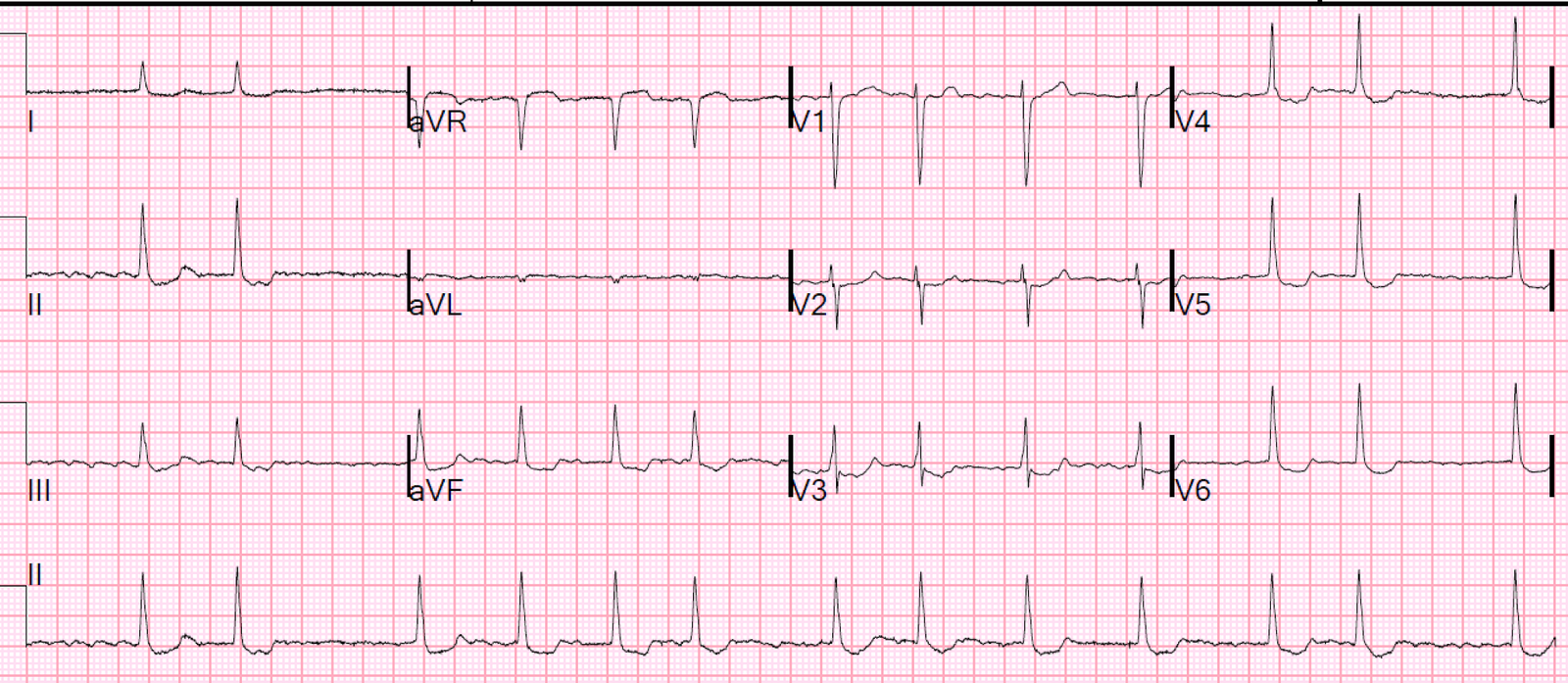
Here the heart rate is obviously no longer 140
What do you think?
ECG: it certainly appears to be an anterior STEMI, but it is important to realize that right ventricular ischemia from either inferior and RV STEMI or from pulmonary embolism can manifest with STE in V1-V3.
On arrival, she immediately lost pulses. Due to body habitus, an adequate transthoracic echo could not be done. There was no ventricular fibrillation recorded, but in the rush of action, she did get defibrillated. Most involved agree there was never any ventricular fibrillation.
This turned out to be a pulmonary embolism (on autopsy).
Massive PE can have Right Ventricular ischemia resulting in RV ST Elevation. When there is sudden loss of pulse but no ventricular fibrillation, then STEMI is an unlikely etiology of arrest. In this series of 1246 cardiac arrests, 60 of which were from PE, only 3 had ventricular fibrillation.
In contrast, the vast majority of initial rhythms in cardiac arrest from acute coronary syndrome are shockable rhythms, and the vast majority are ventricular fibrillation.
This case was particularly confusing because CPR was very effective: good pulses, good O2 saturations, good arterial line waveform, non low end tidal CO2. CPR is generally not very effective in pulmonary embolism because of obstruction of the pulmonary vasculature. Additionally, transesophageal echo (TEE) was placed and did not show a particularly enlarged RV.
Unfortunately, in spite of administration of 100 mg of tPA, the patient could not be resuscitated.
See this case:
Syncope, Shock, AV block, Large RV, “Anterior” ST Elevation….
Learning Points:
1. When there is chest pain and ST elevation in the right precordial leads, think of pulmonary embolism.
2. When there is extreme sinus tachycardia, ACS becomes less likely unless there is:
A. Another simultaneous pathology
B. Pre-existing poor ventricular function or
C. Cardiogenic shock caused by the ACS, and confirmed by poor LV function on bedside cardiac echo.
3. Corollary to Learning point #2.: Cardiac ultrasound and volume assessment is essential to interpreting the ST Elevation on the ECG.
4. If a patient has cardiac arrest witnessed to be PEA, then ACS is very unlikely to be the etiology.
5. If a patient is found in PEA after a significant down time, the arrest may have started as ventricular fibrillation and degenerated to PEA. Such arrests may be due to any etiology.