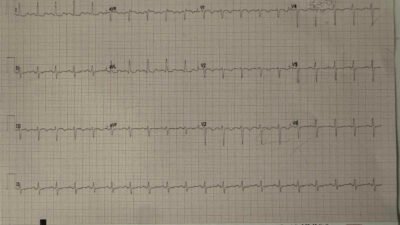
See the ECG before context:
= = =
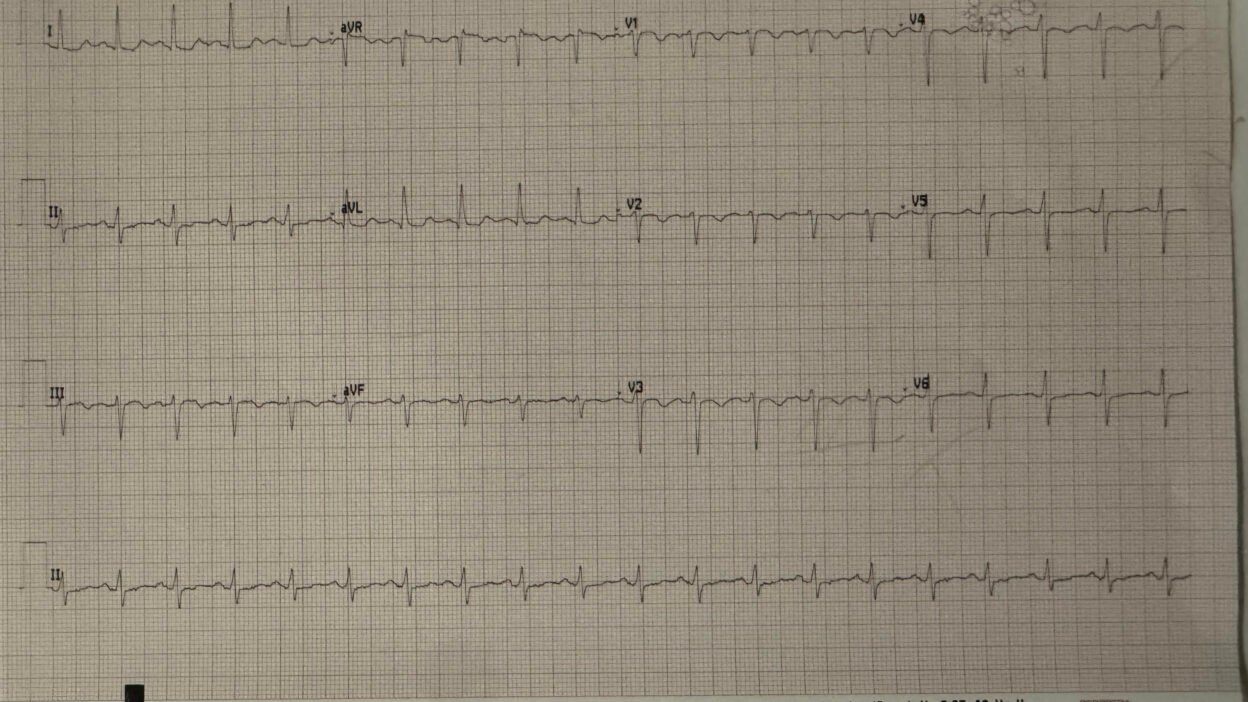
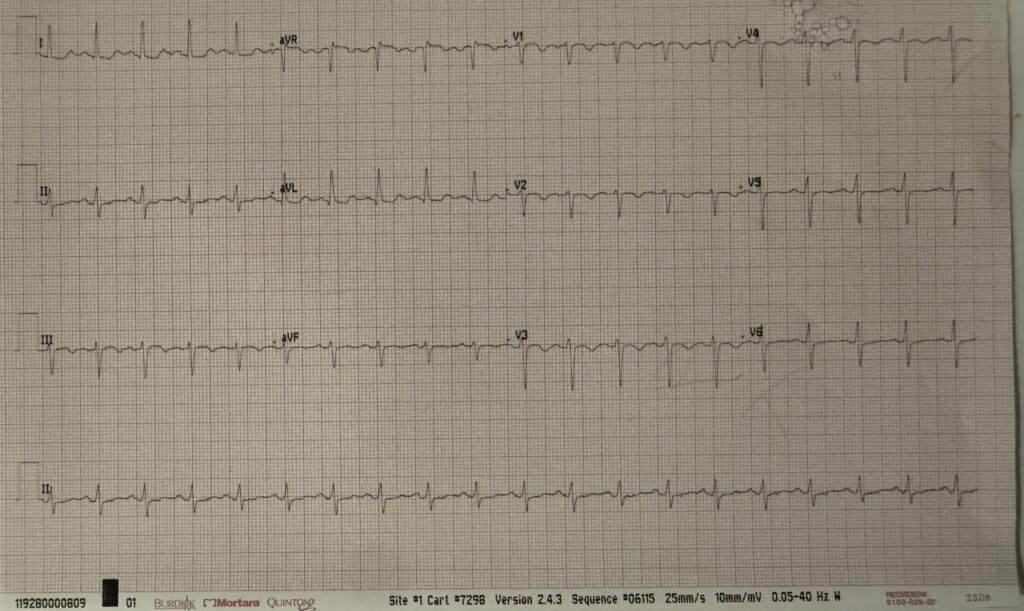
A woman in her 40s presented with shortness of breath and chest pain. She was tachycardic but other vital signs were within normal limits, but she appeared very ill. Her triage ECG is above.
One of my many excellent former residents took care of this patient and recognized the signs of acute right heart strain on the ECG, with the highly specific pattern of simultaneous TWI in inferior and anterior leads, with the correct subjective morphology which is easier to memorize than to describe, but usually includes V2-V4 with small r big s followed by convex ST segment into TWI. Tachycardia makes the diagnosis even more specific.
He performed immediate bedside ultrasound and found a severely dilated right ventricle.
Smith: a severely dilated RV on bedside echo can be pulmonary embolism or chronic right ventricular hypertrophy (RVH). But this ECG tells you that this one is PE! RVH is chronic and, in contrast to acute right heart strain, has a large R-wave in lead V1. V1 is positioned directly over the right ventricle (RV), and an RV that has been pumping against high pulmonary artery pressures for years becomes hypertrophied, which manifests as high positive voltage on an overlying lead. See links below to cases of RVH.
He started heparin and rapidly got CT pulmonary angiogram confirmation of saddle PE.
The patient did well.
= = =
See some of the many other acute right heart strain / pulmonary embolism cases:
A crashing patient with an abnormal ECG that you must recognize
A woman in her 40s with acute chest pain and shortness of breath
A man in his 50s with shortness of breath
Another deadly triage ECG missed, and the waiting patient leaves before being seen. What is this nearly pathognomonic ECG?
A man in his 40s with RUQ abdominal pain
A woman in her 50s with shortness of breath
When the ECG is more revealing than the HPI
A crashing patient with an abnormal ECG that you must recognize
A man in his 40s with a highly specific ECG
Chest pain, ST Elevation, and tachycardia in a 40-something woman
Repost: Syncope, Shock, AV block, RBBB, Large RV, “Anterior” ST Elevation in V1-V3
A young woman with altered mental status and hypotension
A 30-something woman with chest pain and h/o pulmonary hypertension due to chronic pulmonary emboli
A 30-something with 8 hours of chest pain and an elevated troponin
Syncope, Shock, AV block, Large RV, “Anterior” ST Elevation….
Dyspnea, Chest pain, Tachypneic, Ill appearing: Bedside Cardiac Echo gives the Diagnosis
Chest pain, SOB, Precordial T-wave inversions, and positive troponin. What is the Diagnosis?
Cardiac Ultrasound may be a surprisingly easy way to help make the diagnosis
Answer: pulmonary embolism. Now another, with ultrasound….
This is a quiz. The ECG is nearly pathognomonic. Answer at bottom.
Chest Pain, SOB, anterior T-wave inversion, positive troponin
Anterior T wave inversion due to Pulmonary Embolism
Collapse, pulse present, ECG shows inferior OMI. Then there is loss of pulses with continued narrow complex on the monitor (“PEA arrest”)
What do you suspect from this ECG in this 40-something with SOB and Chest pain?
= = =
Cases of RVH:
Syncope, Hypotension, and a Large Right Ventricle — What is the ECG Diagnosis?
Chronic Right Ventricular Hypertrophy, or Acute Right Heart Strain? The ECG Helps Make the Diagnosis.
21 yo F with Syncope has Right Ventricular Hypertrophy and Pulmonary Hypertension
Severe Right Ventricular Hypertrophy
COPD exacerbation, followed by cardiac arrest.
= = =
======================================
MY Comment, by KEN GRAUER, MD (2/25/2026):
An essential component of optimal emergency medicine ECG interpretation is pattern recognition. Although getting a good history — being systematic — correlating the timing of ECGs to the patient’s symptoms are all important — it’s hard to beat the instant recognition of a Brugada-1 tracing, hyperkalemia, shark-fin ST elevation, fascicular VT, and a few other select emergency ECG diagnoses that are most often immediately diagnostic to an experienced clinician who knows what to look for.
- Today’s case provides another prime example of this type of pattern recognition — in which even before knowing the history — Dr. Meyers, Smith and myself all knew within seconds of seeing today’s ECG that the diagnosis of acute PE (Pulmonary Embolism) would be likely until we could prove otherwise.
= = =
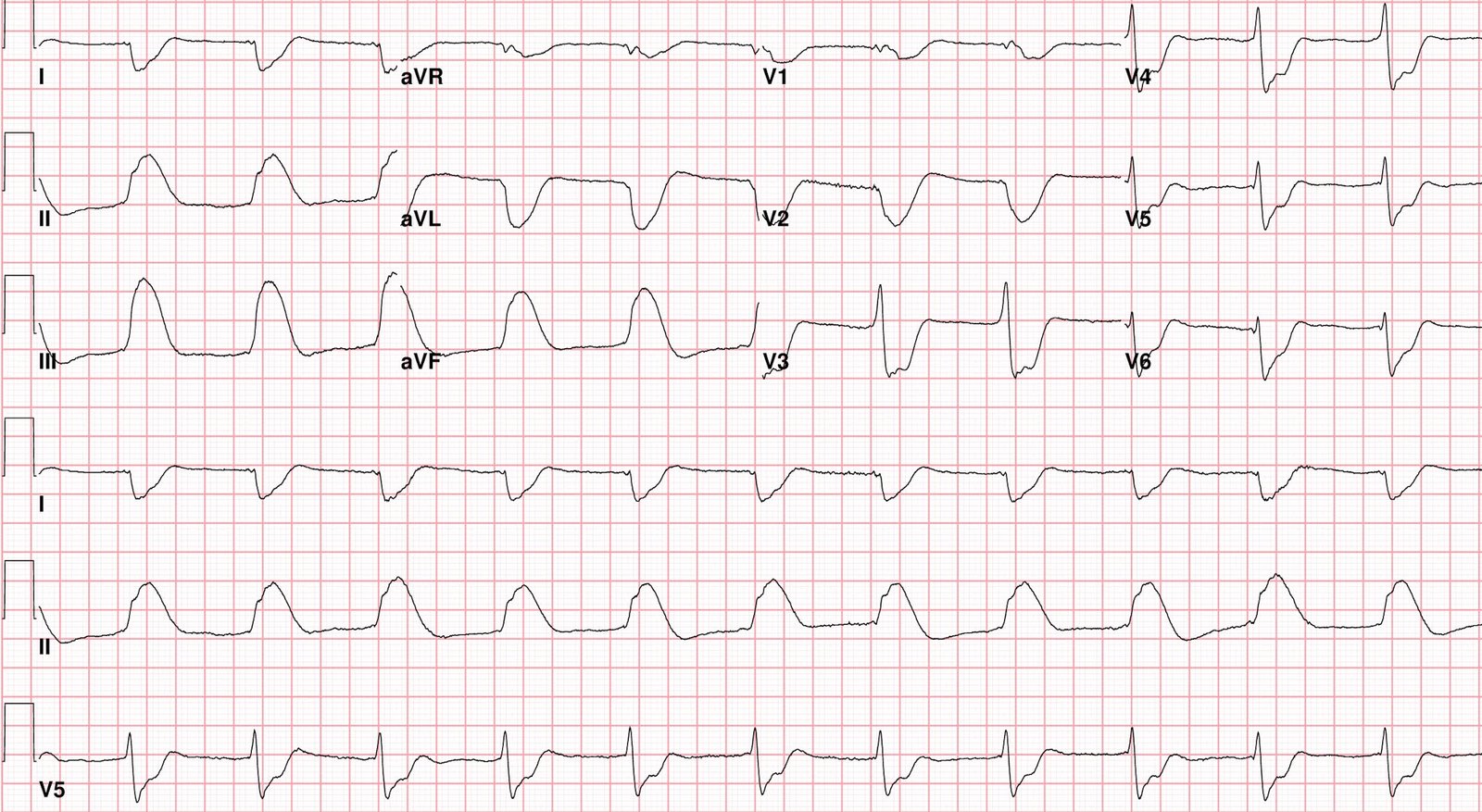
Today’s ECG …
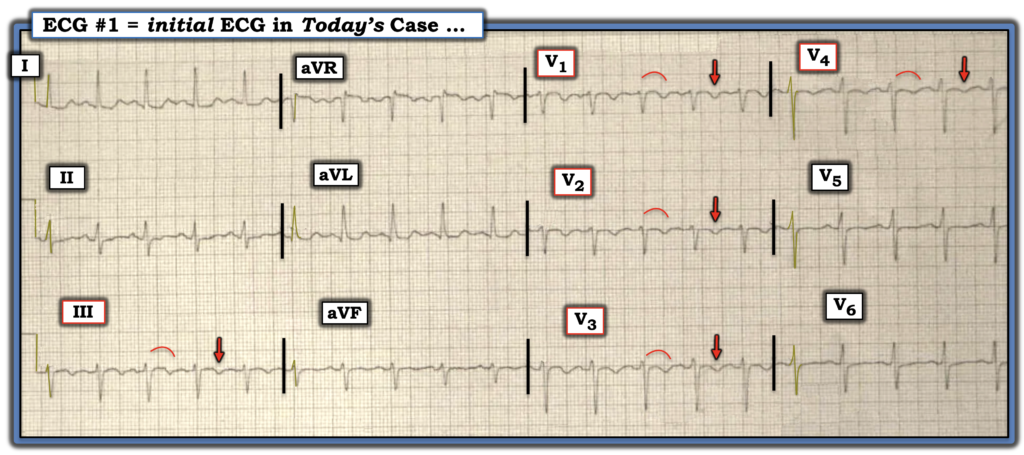
For clarity in Figure-1 — I’ve reproduced and labeled today’s ECG. The incriminating findings implicating acute PE are the following:
- Sinus tachycardia (here at ~115/minute).
- Symmetric T wave inversion in the anterior chest leads (ie, in leads V1-thru-V4 in Figure-1) — and in lead III. Adding to the highly suggestive appearance of acute PE — is the presence of ST segment coving without ST elevation that is seen just before the T wave inversion in these leads.
PEARL: As emphasized by Drs. Smith and Meyers on many occasions: When there is T wave inversion in the anterior chest leads — IF T wave inversion is seen in both lead V1 and lead III ==> Think acute PE (and not acute coronary disease).
- The clinical presentation of acute PE is multifaceted (Boey et al — Singapore Med J 56(10):533-537, 2015). Part of the reason for this is that under the umbrella term of “pulmonary embolism” — there may be: i) Massive PE (in which life-threatening hypotension, if not shock is seen); — vs — ii) Submassive PE (in which there is RV “strain”, often with RV dilatation — but not hypotension); — vs — iii) The broad, much better prognostic category of “lower-risk” PE (in which there is no hypotension — and the range of symptoms and ECG findings is great).
- As might be expected — instant ECG diagnosis of acute PE until proven otherwise is most commonly associated with either massive PE — or the submassive PE that was seen in today’s case.
- Fortunately — the emergency provider in today’s case instantly recognized the diagnosis of acute PE as soon as he saw: i) The ECG in Figure-1; — and — ii) This acutely ill patient, whose presenting symptoms were chest pain and shortness of breath.
KEY Point: Time was not wasted in today’s case chasing the chest pain and anterior T wave inversion for acute coronary disease because this patient’s dyspnea (and tachypnea), in association with marked tachycardia and the ECG finding of ST segment coving with T wave inversion in both lead V1 and lead III are so convincing.
- Bedside Echo performed within the next few minutes — showed a severely dilated RV that: i) Confirmed the diagnosis of acute PE (and the need for prompt anticoagulation); — and — ii) Confirmed that the ECG finding of anterior T wave inversion was not the result of acute coronary disease.
- Saddle PE was seen on CT pulmonary angiogram.
- And as per Dr. Meyers — the patient did well.
= = =
Figure-1: I’ve labeled today’s ECG.
= = =
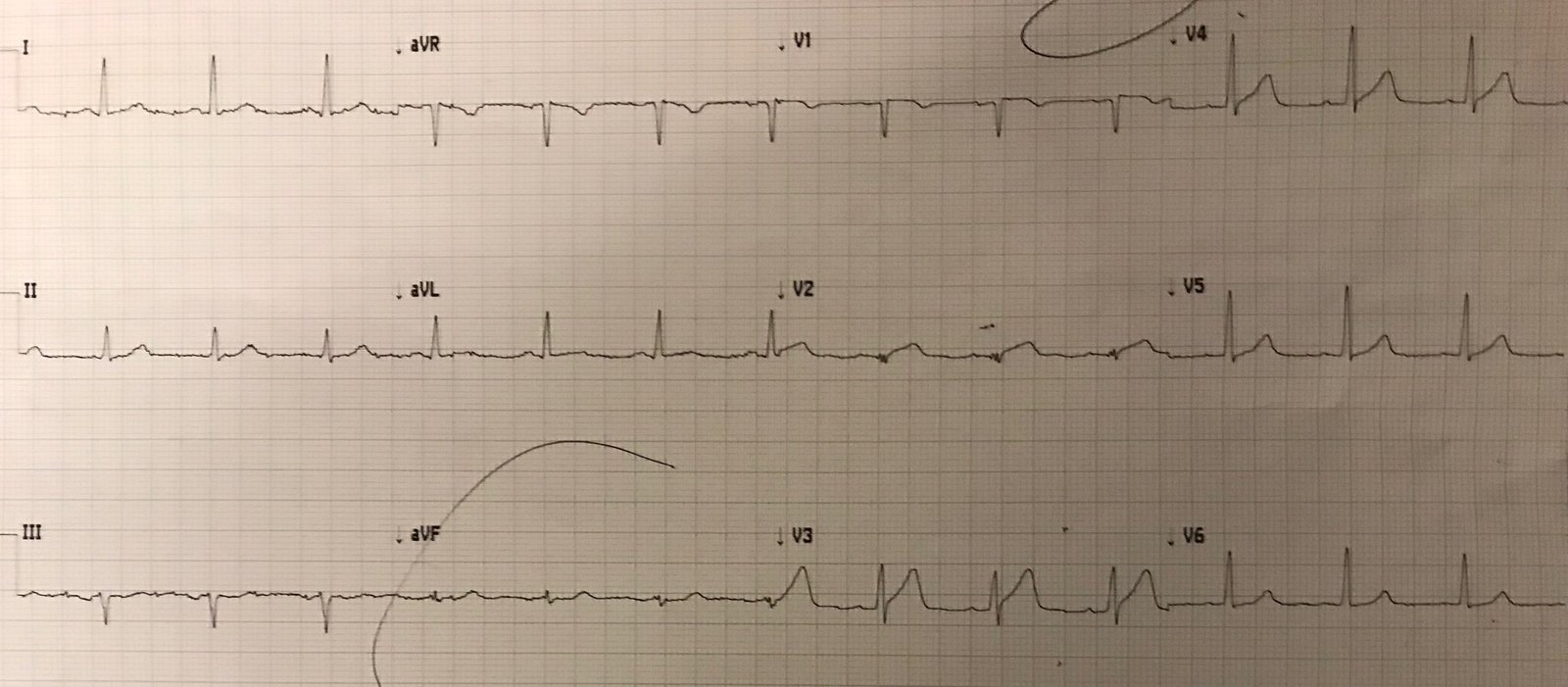
Additional ECG Findings of Acute PE:
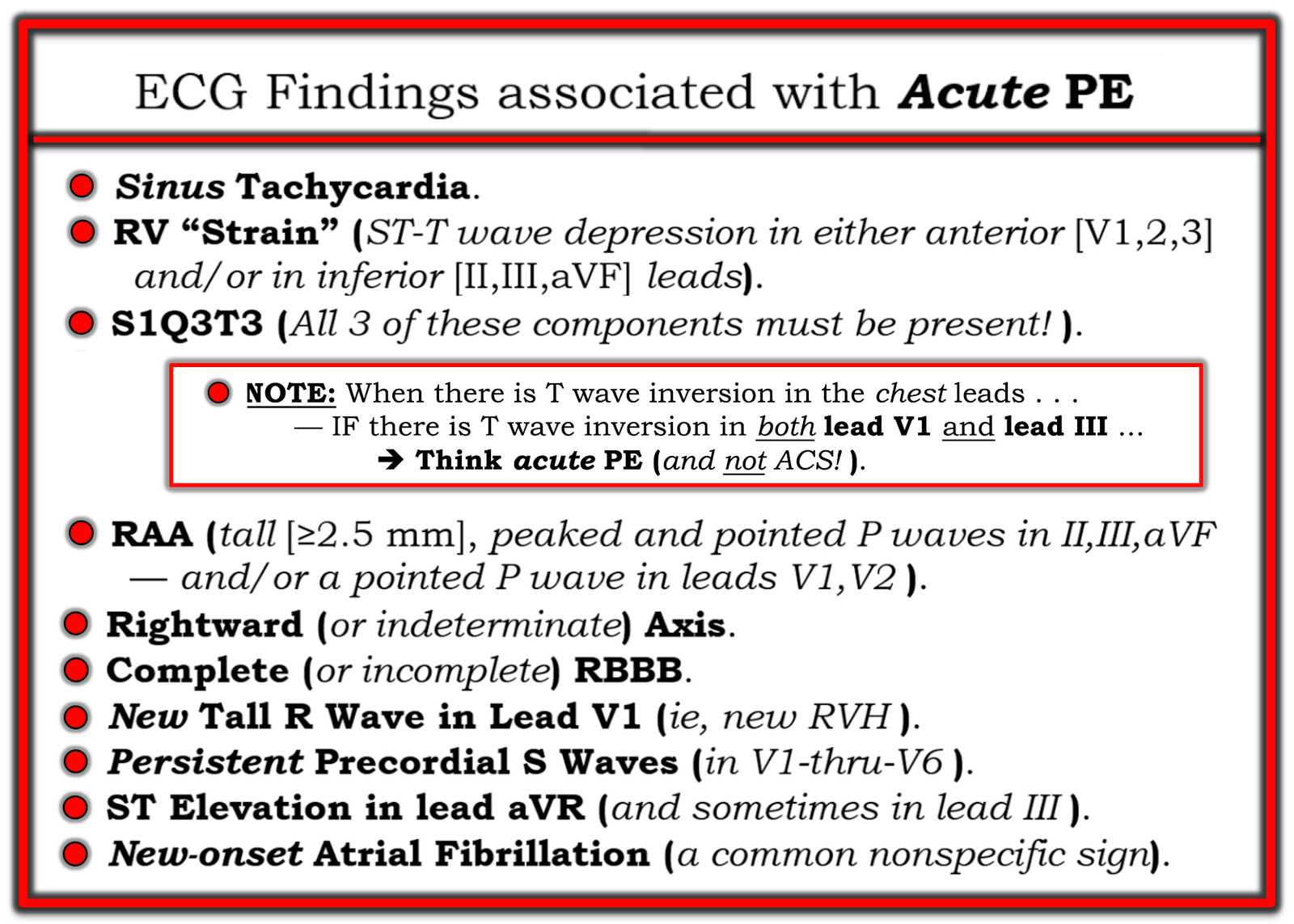
Among the 20+ links to other cases of acute PE noted above by Dr. Meyers — I’ll highlight the November 21, 2024 post — in which I summarize additional ECG findings that may be associated with acute PE (Figure-2 below — that I’ve excerpted from My Comment in this 11/21/2024 post).
- I found today’s case interesting in that the only 2 additional ECG findings from Figure-2 that are seen in today’s ECG are: i) Persistence of S waves throughout the chest leads; — and, ii) A limited amount of ST elevation in lead aVR.
- Missing are right axis deviation — RAA — complete (or incomplete) RBBB — and an S1Q3T3 pattern. But those additional ECG findings are not needed for the presumptive ECG diagnosis of acute PE in today’s case, given the worrisome clinical presentation and the ECG findings that we do see of sinus tachycardia with acute RV “strain” (T inversion in anterior chest leads + lead III).
PEARL: There is a literature suggesting that certain ECG findings in patients with acute PE tend to be associated with a more severe course (Shopp et al: Acad Emerg Med 22(10):1127-1137, 2015 — Boey et al: Singapore Med J 56(10):533-537, 2015 — Kukla et al: Am J Emerg Med 32(6):507-510, 2014). These ECG findings include:
- New low voltage.
- Acute RV “strain” (anterior and inferior T wave inversion).
- Complete RBBB.
- ST elevation in lead V1 (and other pseudoinfarction patterns).
- ST elevation in lead aVR.
- Atrial fibrillation and/or other atrial arrhythmias.
- Significant sinus tachycardia.
- S1Q3T3 pattern.
= = =
Figure-2: ECG findings associated with acute PE.
= = =
= = =