|
A middle-aged patient presented with resolved chest pain.
|
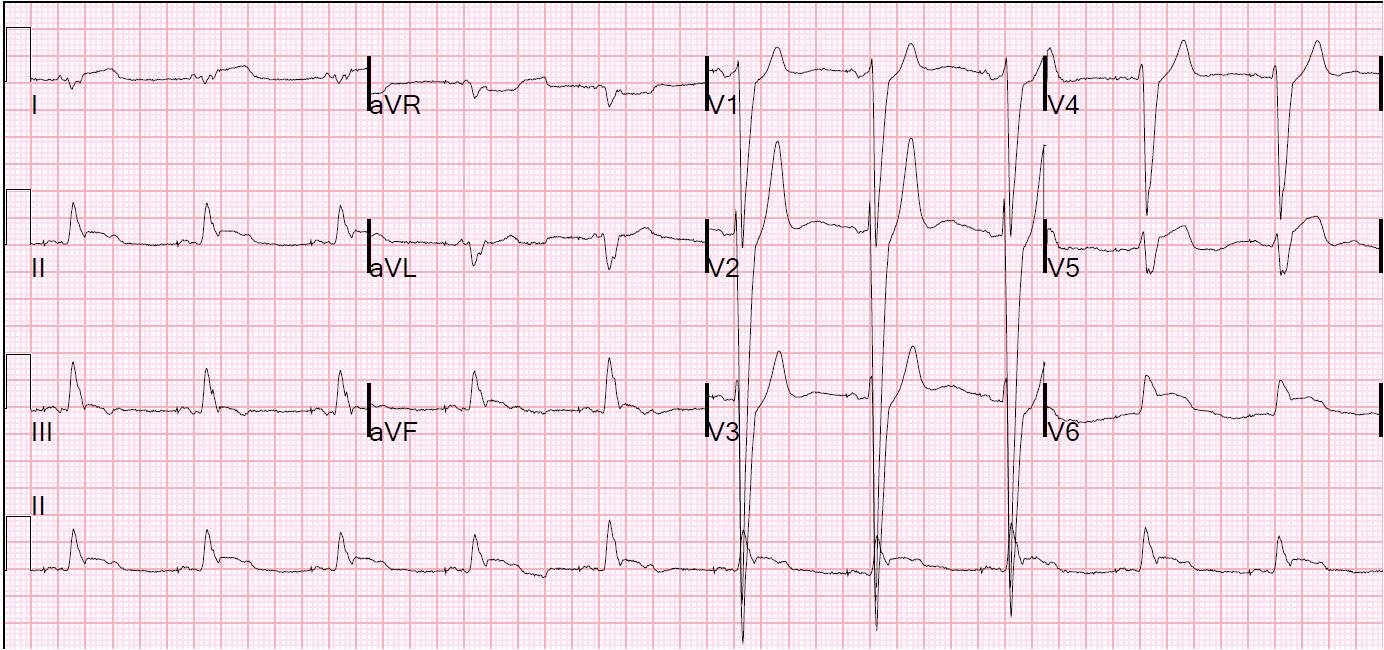
| t = 0, presentation to ED: Initial ECG of 50 yo woman who had prehospital chest pain, now resolved. There is old inferior MI (and the nonspecific minor T inversion in aVL may be due to this, or may be new).
There is subtle ST elevation in V2 and V3 with reverse R-wave progression and subtle ST depression in V5 and V6. This ST elevation should not automatically be attributed to normal variant early repol because there is also reverse R-wave progression and the afore-mentioned STD in V5 and V6, neither of which occur with normal variant ST elevation. Therefore, this is suspicious for resolving LAD occlusion. Serial ECGs are critical, especially if chest pain persists or recurs. |
The patient remained pain free, and did not get another ECG for 110 minutes:
 |
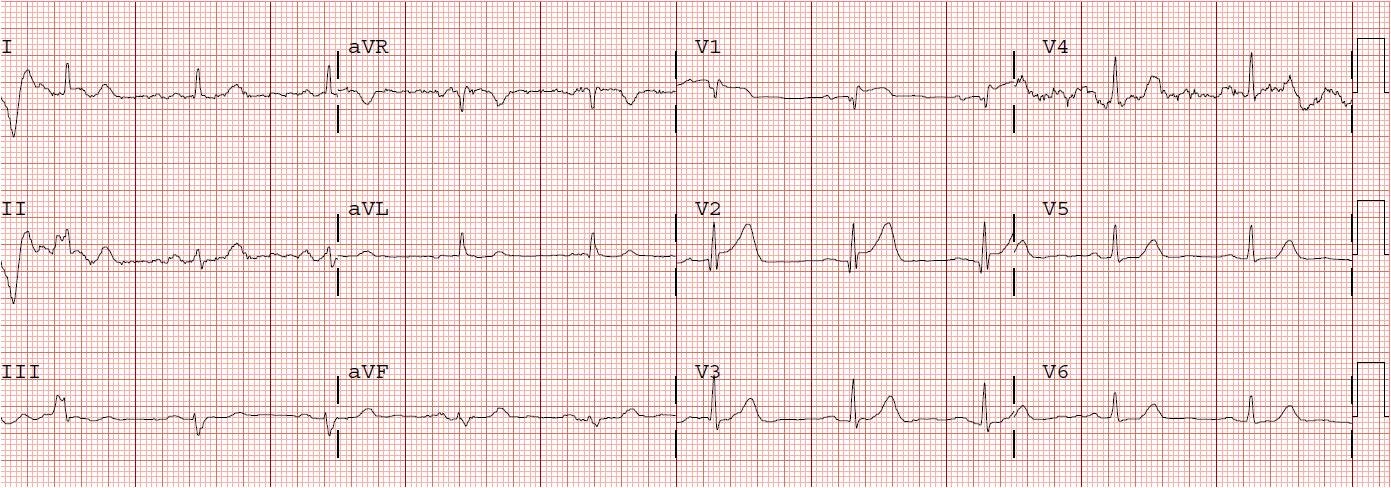
| t = 1.83 hours. There are now the beginnings of T-wave inversion in aVL, V4 and V5. |
 |
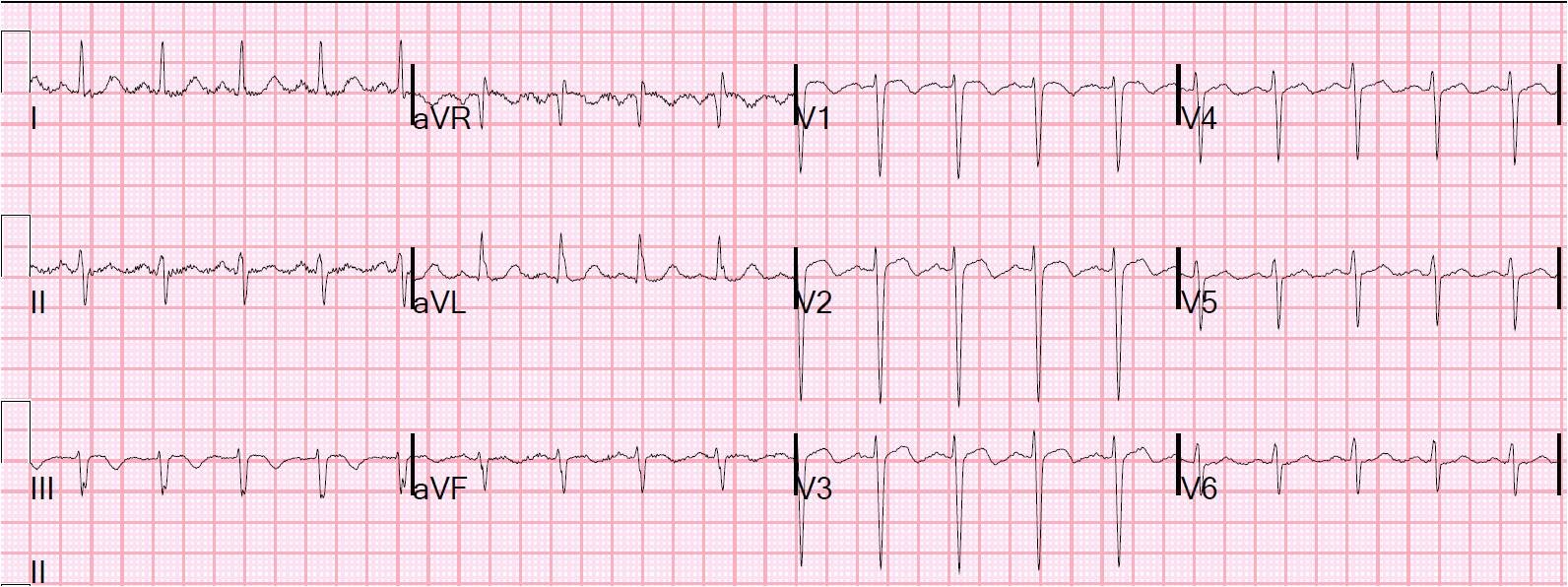
| t = 4.75 hours. Now there is the beginning of T-wave inversion in V2, with more in V3, and progressive T-wave inversion in aVL, V4, and V5. |
 |
| t = 6 hours. Still more T-wave inversion, becoming symmetrical in V4 and V5. |
 |
| t = 8.5 hours. Still more T-wave inversion and increasing symmetry. |
 |
| t = 23 hours. Deepening T-waves with increasing symmetry. |
 |
|||||||
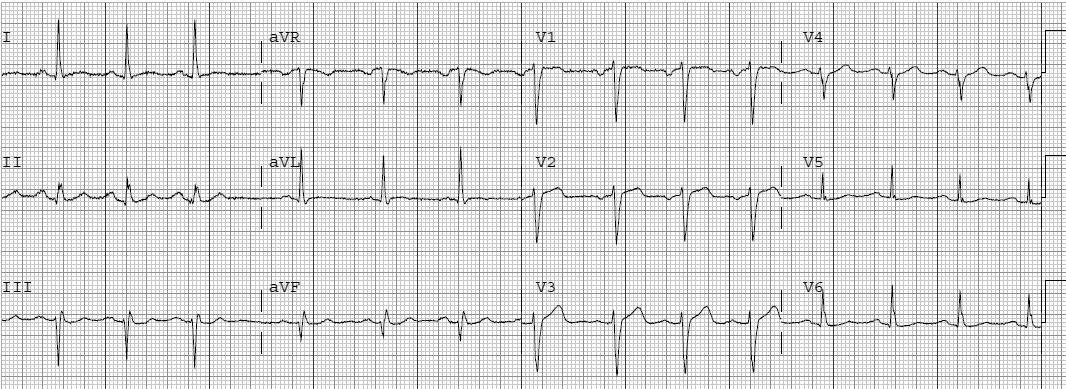
| t = 27 hours. Diffuse symmetric T-wave inversion. The patient had positive troponins and a tight LAD stenosis that was stented. |