by Jesse McLaren
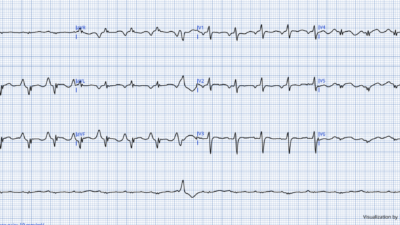
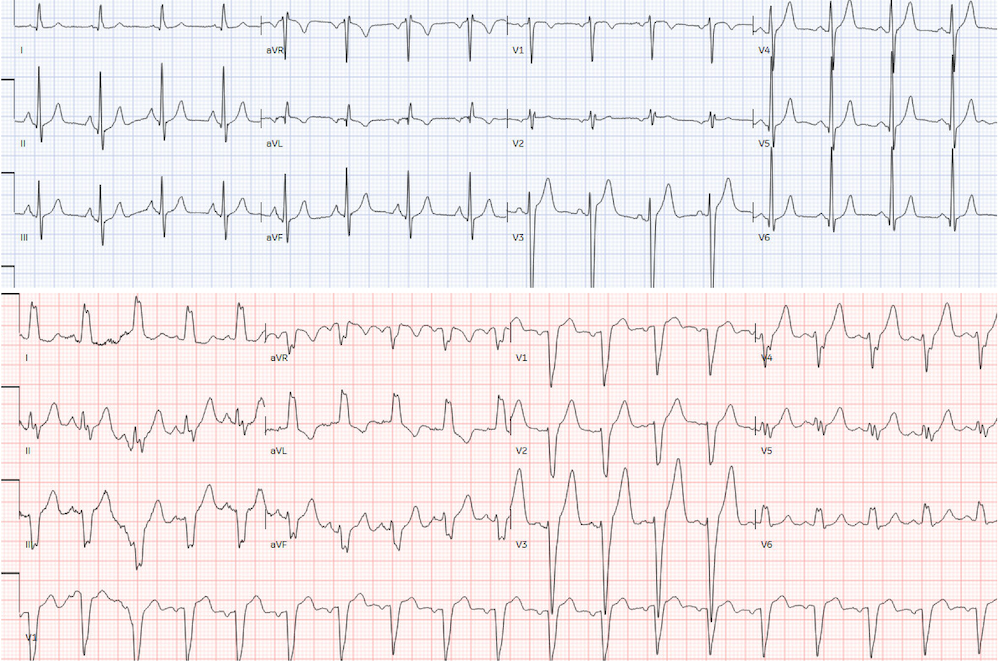
A 65 year old with a history of COPD, coronary artery disease, reflux and cocaine use presented with chest tightness and shortness of breath for a few days. Triage heart rate was 107, BP 150/90, respiratory rate 20, saturation 98% on room air, and afebrile. ECG showed a LBBB which was new compared to the previous one just 10 days prior (when the patient presented with mild shortness of breath with unremarkable investigations). Below is the prior and new ECG: should the cath lab be activated for this patient with chest pain and new LBBB?
.
.
.
There’s baseline wander in the limb leads, sinus tachycardia a new LBBB. There is no Modified Sgarbossa Criteria on the ECG (no concordant STE, concordant STD V1-3, or excessive discordant STE), and the patient was hemodynamically stable without such a high pre-test probability to diagnose OMI on clinical grounds. But because of chest pain and ‘new LBBB’ the emergency physician called a code STEMI.
Smith: the heart rate on the top ECG is slightly below 100; the rate on the bottom one is slightly above 100. Rate-related BBB is possible here. What is rate-related BBB? Rate-related BBB means that the refractory period of the bundle branch at baseline is longer than normal, and at an increased heart rate, it does not have time to repolarize and so is functionally blocked, even though is might work fine at a slower rate. See cases below.
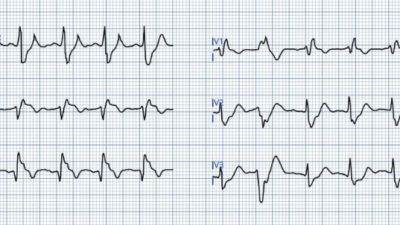
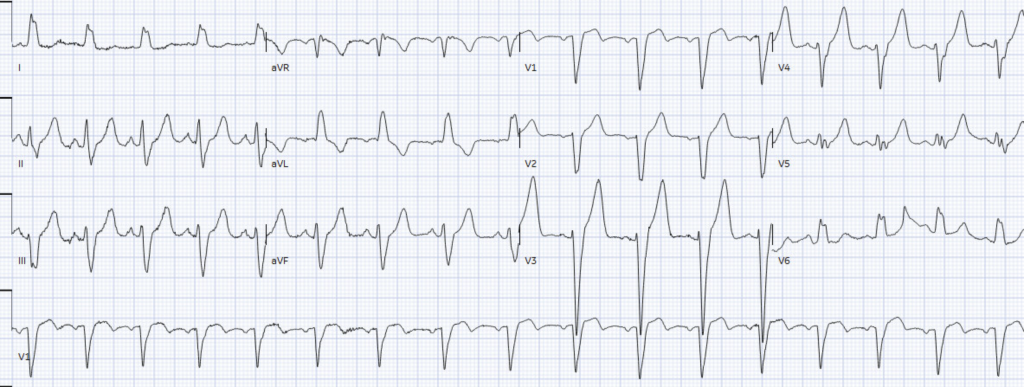
Cardiology repeated the ECG, which showed resolution of baseline wander and still no superimposed ischemic changes:
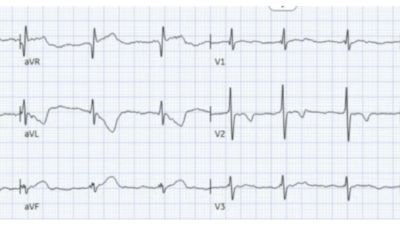
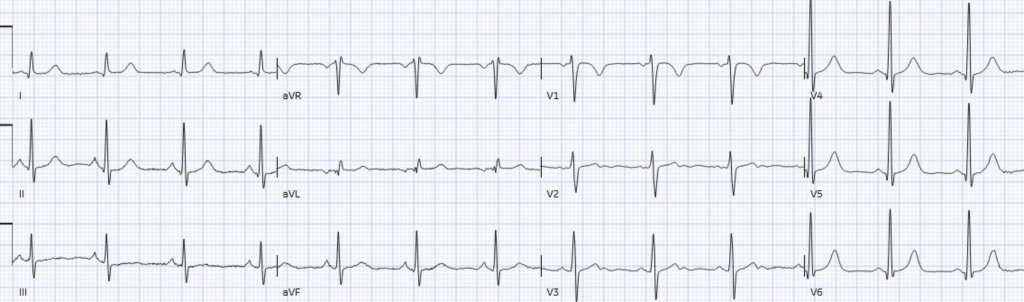
Cath lab was canceled, and CT chest showed no aortic dissection but the presence of pneumonia. Labs showed a normal troponin and potassium level, and elevated WBC. The patient improved on antibiotics, and the discharge ECG showed resolution of the LBBB:
Second visit next year: another ‘new LBBB’
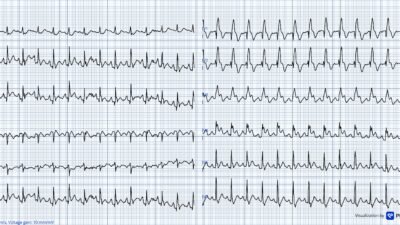
The next year the patient presented with 6 hours of chest pain, nausea and vomiting, which improved with nitro spray. Vitals were normal and ECG showed new LBBB compared to the prior discharge ECG.
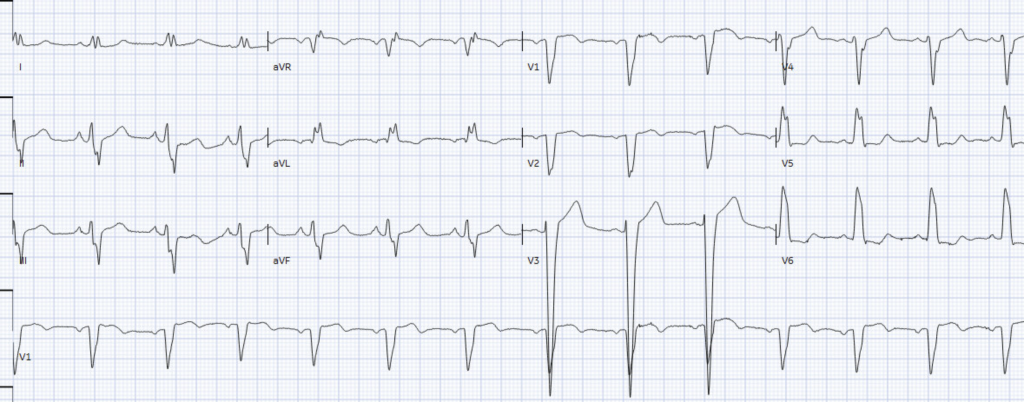
This time the emergency physician documented negative (Smith-modified) Sgarbossa criteria. Serial troponins were undetectable, but because of the concerning history the patient was admitted for unstable angina vs cocaine-induced chest pain.
Echo showed EF of 30% with globally reduced function, and angiogram found only a 45% RCA stenosis that did not explain the cardiomyopathy. The patient was diagnosed with cocaine-induced cardiomyopathy and given follow up with addition medicine. LBBB remained on discharge ECG.
From ‘new LBBB’ to Smith-Modified Sgarbossa Criteria
These two visits show the variable treatment of patients with chest pain and LBBB. This reflects a longstanding tug of war between the STEMI paradigm and evidence-based advances:
- 1994 thrombolytic trials: thrombolytics for chest pain + BBB (regardless of timing)
- 1996 Sgarbossa study: can differentiate LBBB with vs without MI
- 2000: STEMI defined as STE in the absence of LBBB
- 2004 STEMI guidelines: thrombolytics for ‘new or presumably new LBBB’
- 2012 Smith-Modified Sgarbossa Criteria: can differentiate LBBB with vs without OMI
- 2013 STEMI guidelines: ‘new LBBB’ is not STEMI equivalent, but no mention of Modified Sgarbossa
- 2015 and 2021: validation of Modified Sgabossa in LBBB and paced rhythms
- 2022 ACC expert consensus: recognizes Smith-Modified Sgarbossa
- 2023 ESC ACS guidelines state that LBBB or paced rhyhtm “precludes an accurate assessment of the presence or absence of ST-segment elevation”
- 2025 ACC ACS guidelines: no mention of Modified Sgarbosa Criteria, instead “new or presumably new LBBB at presentation occurs infrequently and should not be considered diagnostic of AMI in isolation; clinical correlation is required.”
- 2025 systematic review and meta-analysis: LBBB chronology has no diagnostic impact, whereas Modified Sgarbossa Criteria has high sensitivity and very high specificity
De Alencar found from 51 studies that ACS with LBBB had higher in-hospital mortality, but the chronology of LBBB was diagnostically neutral (with LR+ and LR- that crossed the null value of 1.0). In contrast, the Modified Sgarbossa Criteria had LR+ of 11.3 and LR- of 0.18, so it can differentiate LBBB with vs without OMI (unless the patient has a very high pre-test likelihood, where the ECG has insufficient sensitivity for OMI regardless of LBBB).
(See the systematic review and meta-analysis by de Alencar here; and editorial by McLaren, Helseth and Smith here)
Take home
- ‘New LBBB’ does not identify patients with acute coronary occlusion.
- LBBB does not preclude assessment of presence or absence of ECG signs of OMI
- The Smith-Modified Sgarbossa Criteria can identify OMI in the presence of LBBB or paced rhythms
- Very high pre-test likelihood ACS (eg refractory ischemia or hemodynamic/electrical instability) requires angiography regardless of the ECG
- Remember Rate-related Bundle Branch Block
Here is a fascinating case of rate-related LBBB which also shows “cardiac memory”: Chest pain and LBBB. LBBB resolves and there is V1-V3 T-wave inversion.
= = =
==================================
MY Comment, by KEN GRAUER, MD (5/25/2026):
I found today’s case by Dr. McLaren a fascinating illustration of variations on LBBB (Left Bundle Branch Block).
- The 65-year old patient has a bit of “everything” — including:
- Pulmonary disease (from known COPD — and an episode of CT scan-verified pneumonia requiring hospital admission for IV antibiotics — but another ED visit for similar shortness of breath with negative investigations);
- A longterm history of Cocaine abuse (thought to be the cause of a cocaine-induced cardiomyopathy — as well as a source of this patient’s intermittent chest pain);
- Significant underlying heart disease (with a label of “coronary artery disease” — globally reduced LV function with an Echo-determined EF of ~30%, but only 45% RCA narrowing on his most recent cath — and hard-to-explain symptoms over time, including chest “tightness” and chest pain responding to nitroglycerin).
- And — a series of ECGs showing intermittent LBBB.
= = =
The Patient’s Intermittent LBBB …
Over the course of Dr. McLaren’s interesting presentation — this patient had 5 ECGs — with 3 of the 5 showing LBBB, but 2 of the 5 without this conduction defect!
- The finding of intermittent LBBB — suggests a component of a rate-related conduction defect. But although the first 4 ECGs shown comply with the dogma that rate-related LBBB will be seen when the heart rate is faster and resolve when the rate slows — the 5th ECG shows persistence of LBBB despite a modest heart rate of only ~80/minute.
- The significance of LBBB depends on “the company it keeps”. In this patient with the above described complex history — his intermittent LBBB is most likely a consequence of this patient’s documented cardiomyopathy. But intermittent rate-related LBBB may also occur simply as a consequence of a tachyarrhythmia in the absence of any underlying heart disease. In contrast — Patients with persistent LBBB almost uniformly have some form of significant underlying heart disease.
- LBBB conduction is important clinically — because it not only alters the sequence of ventricular depolarization, but also of ventricular repolarization, thereby posing difficulty for distinguishing between ST-T wave “abnormalities” due to acute ischemia vs simply being the result of the conduction defect. Modified-Smith-Sgarbossa Criteria provide great assistance in assessing ST-T wave changes in patients with LBBB — but the criteria are not perfect.
- PEARL: For any form of rate-related conduction defect (ie, including rate-related LBBB, RBBB, and hemiblock forms) — the rate of onset of BBB conduction is often not the same as the rate where normal conduction resumes (ie, rate-related BBB may begin when heart rate exceeds 90 or 100/minute — but normal conduction may not resume until heart rate goes back down to 80/minute or less). As might be imagined — this truism about the potential difference between the rate of “onset” vs “offset” of rate-related BBB can sometimes make it difficult to determine if your patient has an underlying impaired conduction system defect vs a purely rate-related phenomenon.
= = =
Assessing ST-T Waves in Today’s Case:
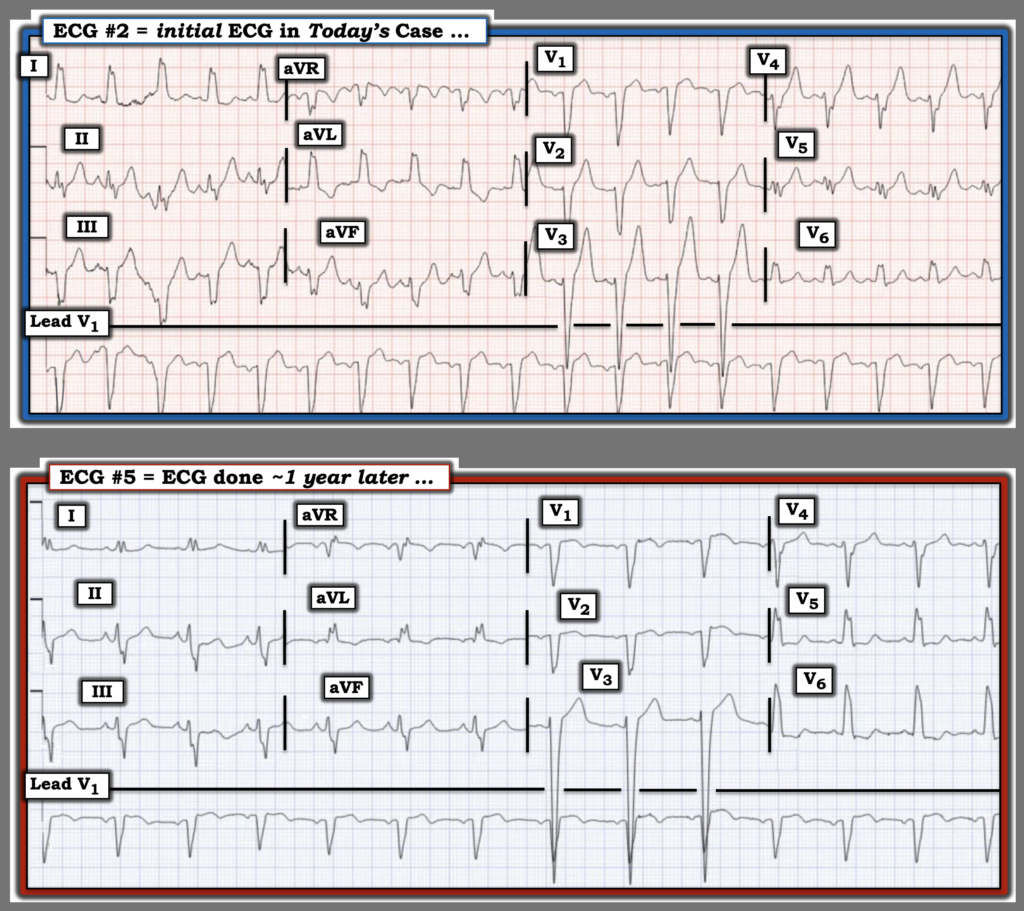
Take another LOOK at 2 of today’s 5 ECGs — that for clarity, I’ve put together in Figure-1.
- Both of the ECGs in Figure-1 show sinus rhythm with LBBB. Neither demonstrates an inappropriate amount of J-point ST elevation (ie, >25% of the depth of the preceding S wave).
- = = =
- QUESTION: Is there a qualitative difference in ST-T wave appearance between the 2 tracings?
= = =
Figure-1: I’ve reproduced the 2nd and 5th ECGs in today’s case.
= = =
My Thoughts:
When I first reviewed today’s case — I was concerned about the ST-T wave appearance in leads V4,V5,V6 in ECG #2.
- While true that the ST-T waves in leads V2 and V3 of ECG #2 are clearly more peaked than they are in ECG #5 — I thought this to be non-diagnostic, given LBBB and minimal J-point ST elevation.
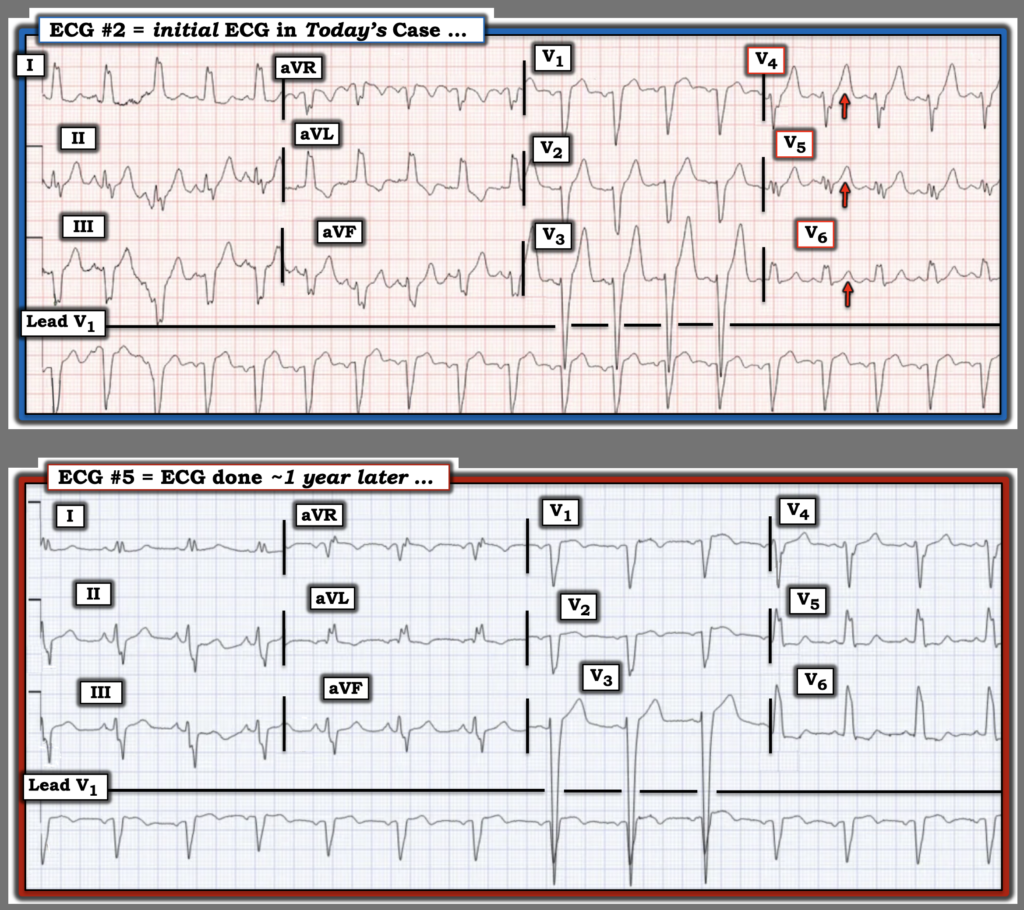
- Qualitatively however (as I highlight below in Figure-2) — I thought the ST-T waves in leads V4,V5 of ECG #2 were disproportionately enlarged — with an upright T wave in lead V6 that “shouldn’t be upright” given the predominantly upright QRS of LBBB in this lead.
- Given that this patient reported “chest tightness for a few days” at the time that ECG #2 was recorded — I was concerned about the possibility of an acute ischemic process.
= = =
Figure-2: I’ve labeled the leads in ECG #2 that concerned me.
= = =
= = =