For other cases of inferior hyperacute T-wave click here and here.
For more on lead aVL, click here and here. Also use labels on the right sidebar.
Case
A 65 yo woman called 911 for pain in her upper back (between the shoulder blades) and in the left shoulder and left biceps, and some “mild chest pressure” elicited by the medics. Exam was normal. All but the back pain resolved with nitroglycerine
Medics recorded 6 prehospital ECGs. Below are 3 of them:
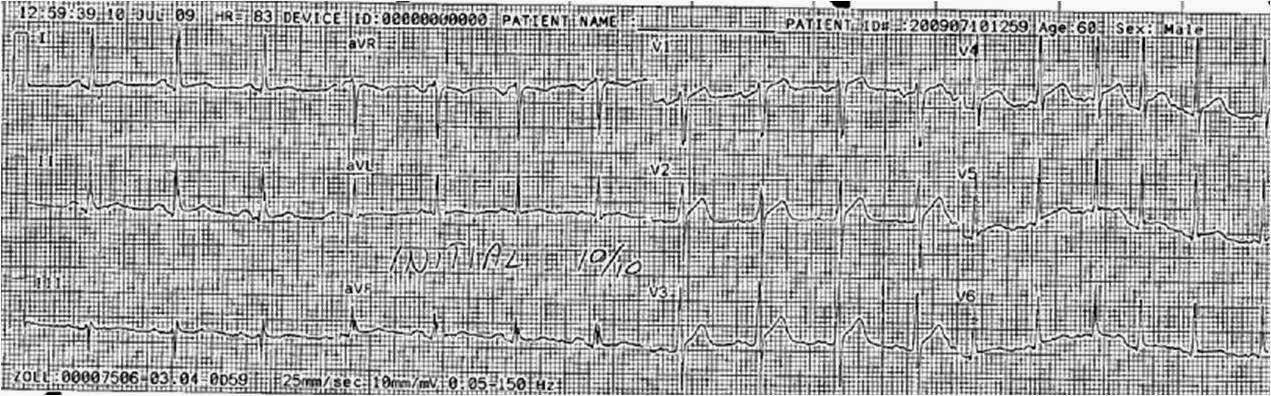
1430
 |
|
|
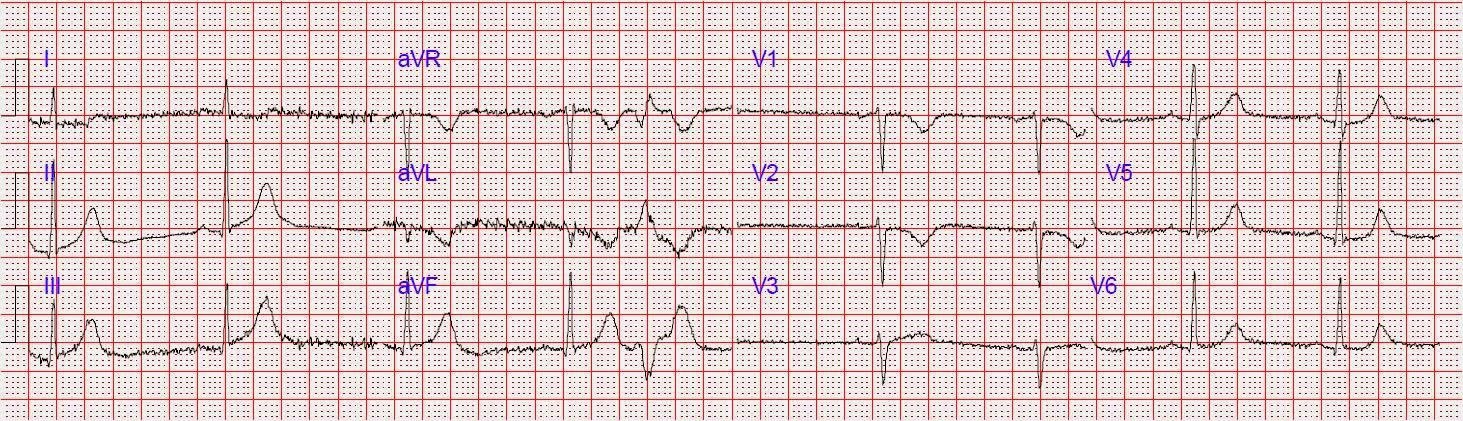
1432
 |
|
|
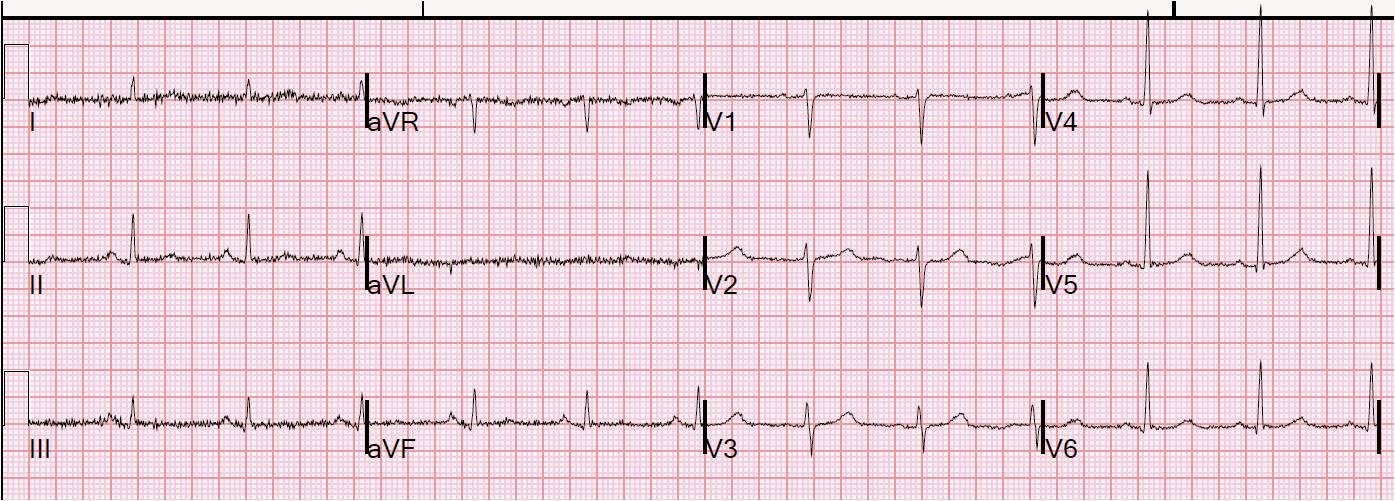
1445
 |
|
|
They arrived in the ED at 1503. BP was 116/70. CXR and cardiac and aortic ultrasound were done to look for any evidence of aortic dissection. All were normal except for a possible inferior wall motion abnormality.
In the ED, the following ECGs were recorded.
1512
 |
|
|
1532
 |
|
|
1542
 |
|
|
Cardiology was consulted. Again, a cardiology fellow opined that this was not a STEMI, and went to talk with the interventionalist.
A posterior ECG was recorded:
 |
|
|
The interventionalist was very concerned and activated the cath lab. The patient was taken to the cath lab. The proximal RCA was 100% occluded. It was stented. Door to balloon time was 62 minutes. Peak troponin I was 5.15 ng/ml.
Post PCI ECG
 |
| T-waves and ST segments are back to normal |