Before we start, here is another popular post on wide complex tachycardia.
What is the ECG rhythm diagnosis?
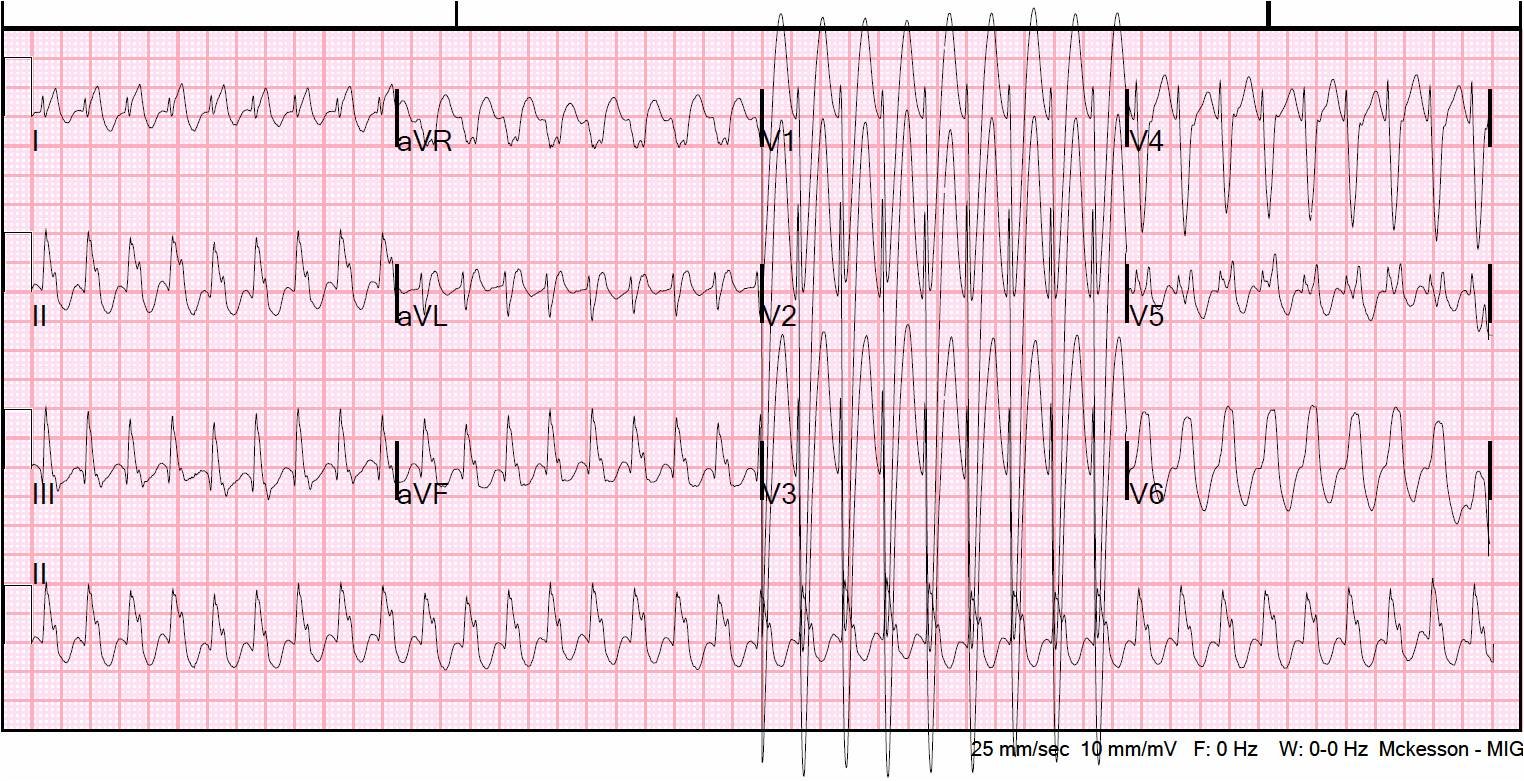 |
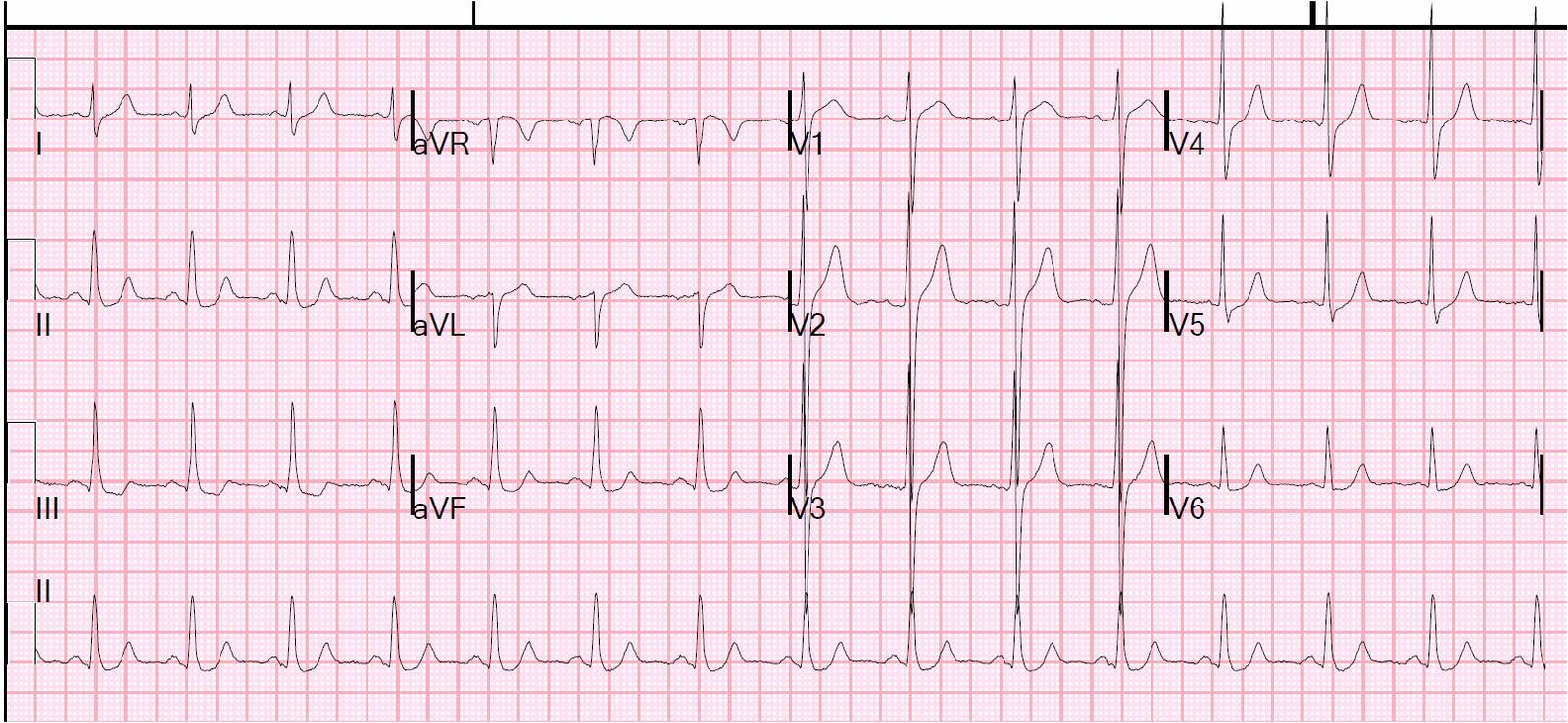
| Wide complex regular tachycardia at a rate of 209, so it is not atrial fibrillation. |
First, in regular wide complex tachycardia: when in doubt, just use electricity, even in stable patients! Electricity is safer than medications and will work no matter the diagnosis. A small dose of propofol is adequate for the patient to be amnestic to the cardioversion.
But even if you can manage it, it may be useful to determine the diagnosis:
Which is it?
1) VT
2) SVT with aberrancy (usually AV nodal reentry tachycardia with aberrancy)
3) AV reciprocating tachycardia [antidromic, up through AV node and down through bypass tract, (AVRT)]4) What can you do if you don’t know? (Does it matter?)
4) I should briefly mention idiopathic VT, which occurs in structurally normal (or nearly normal) hearts, and is therefore not as dangerous as standard VT; this includes adenosine-sensitive VT (RV outflow tract, with LBBB morphology, monomorphic R-wave in inferior leads) and verapamil-sensitive VT (posterior fascicle, RBBB morphology). I will discuss this in a future post.
Here is the clinical data:
26 yo male with chest pain and SOB and no history of structural heart disease. He was not hypotensive or in shock.
A young person with no cardiac history is likely to have SVT, not VT, but let’s consider the ECG alone:
When assessing for the rhythm in wide complex regular tachycardia, these are the assessments I make, though no method is foolproof:
1) Look for hidden p-waves before each QRS. Don’t miss sinus rhythm! Not here.
2) If there is a transition from narrow to wide, is the rate the same? Then it must be SVT. Not here.
3) QRS duration: VT usually (but not always) has a QRS duration of at least 140 ms. A prominent exception is fascicular VT. The longer the QRS, the more likely it is to be VT. Here it is 155 ms, so it is plenty long for VT.
4) Is there RBBB or LBBB morphology and is the initial part of that BBB narrow? Then it is very likely to be SVT. This one has LBBB morphology with a narrow initial R-wave.
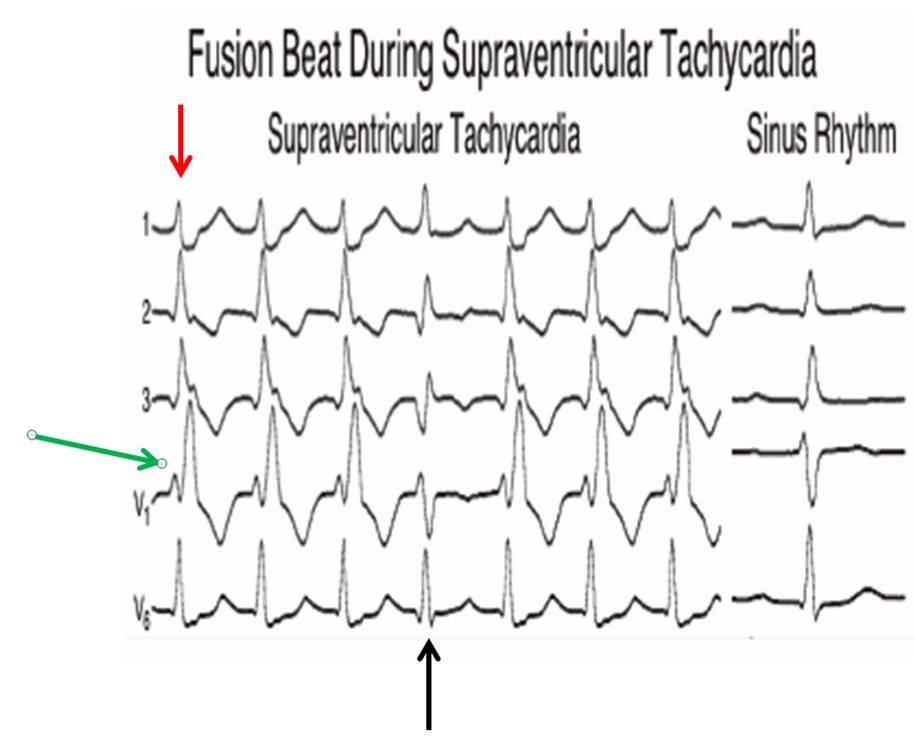
5) Do a quick look for obvious fusion beats and AV dissociation. If found, then VT. None here.
6) Do a quick look for concordance (all QRS’s in the same direction in precordial leads, not the same as concordance when evaluating ST segments in LBBB). Concordance means there is no RS. No concordance here: this is easy to see comparing V4 to V6.
7) Finally, because it is easy to apply, I like a new rule better than Brugada’s or Vereckei #1 or Vereckei #2 (aVR). It is Sasaki’s rule (Sasaki K. Circulation 2009; 120:S671), and it had 86% sensitivity and 97% specificity among 107 cases of wide complex tachycardia. It has not been validated; this is important: remember that Brugada’s rule was much better in the initial study than in subsequent validation studies.
Step 1: Initial R in aVR?
This means is there a large single (upright) R-wave (not a small r-wave) in aVR. This indicates that the beats originate and propagate from the apex to the base, so that it must be coming from the ventricle, hence VT.
–If yes, then rhythm is VT. If no, step 2. Not here.
Step 2: In any precordial lead, is the interval from onset of R-wave to the nadir of the S ≥ 100 msec (0.10 sec)? See image below.
–If yes, then rhythm is VT. If no, step 3. Not here.

Step 3: Initial r or q ≥ 40 ms in any lead?
If there is, this means that, for the first 40 or more milliseconds, conduction is slow as would occur through myocardium (left ventricle, VT), not through conducting fibers, as would occur in SVT)
–If yes, then it is VT. If no, then it is SVT. “No” here, therefore it is SVT
Treat without a diagnosing
If you don’t know what to do, you can always use electricity, but you can also give adenosine. As long as the rhythm is regular, not irregularly irregular (atrial fibrillation), adenosine is safe. It will usually (safely) convert SVT with aberrancy and AVRT (antidromic reciprocating tachycardia) without harming a patient in VT, and may convert a patient with fascicular VT.
Obviously, synchronized cardioversion should be undertaken if the patient is unstable.
If it is irregular with a wide QRS, it could be WPW, in which case an AV nodal blocker could be life threatening (see this post).
Diagnosis: SVT with aberrancy; it resolved with adenosine.
Added Oct 22, 2011: many readers thought this was RV outflow tract VT. The reason that RVOT VT is very unlikely is that RVOT starts in the outflow tract and propagates inferiorly; therefore, inferior leads are all positive. In this case, there is an initial Q-wave in inferior leads.
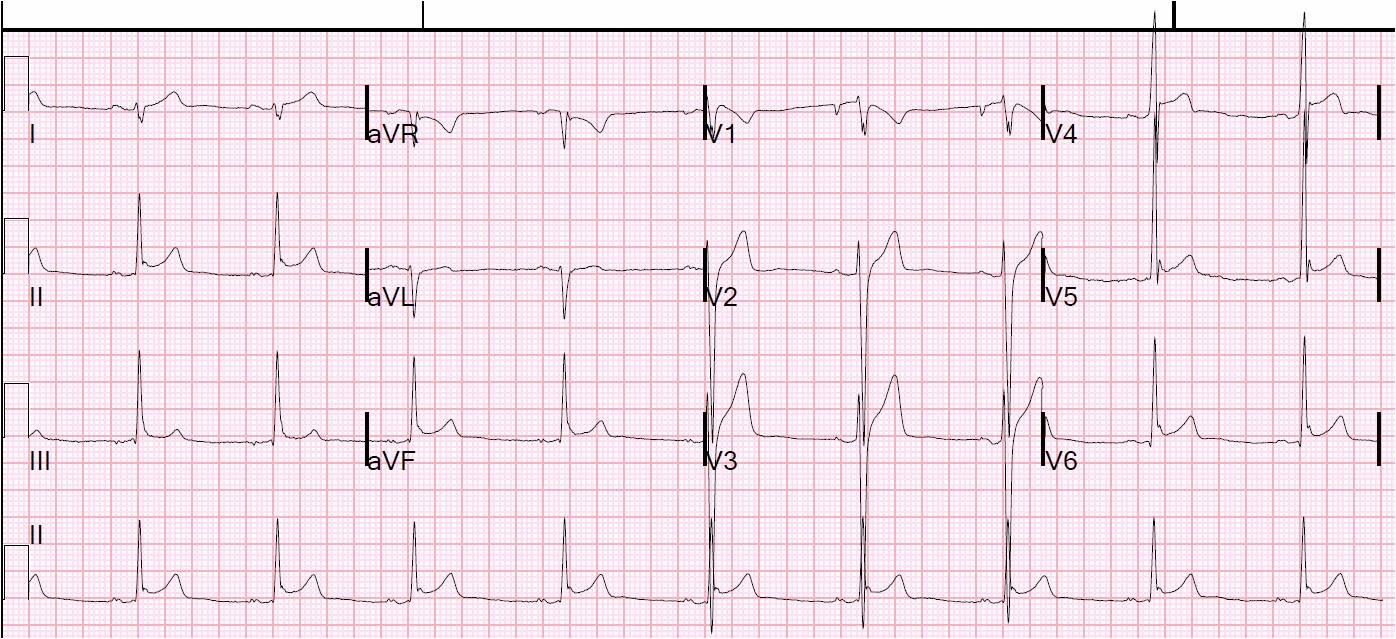
Here is the post-conversion ECG:
 |
| There is slight slurring at the beginning of each QRS, suggestive of delta waves, and the QRS is thus 109 ms (borderline wide). The PR interval is 138 ms, so WPW is very unlikely. There is also some ST depression which appears to be secondary to this slightly abnormal QRS, and lends some further credibility to some sort of pre-excitation. |
There is no further follow-up at this point.