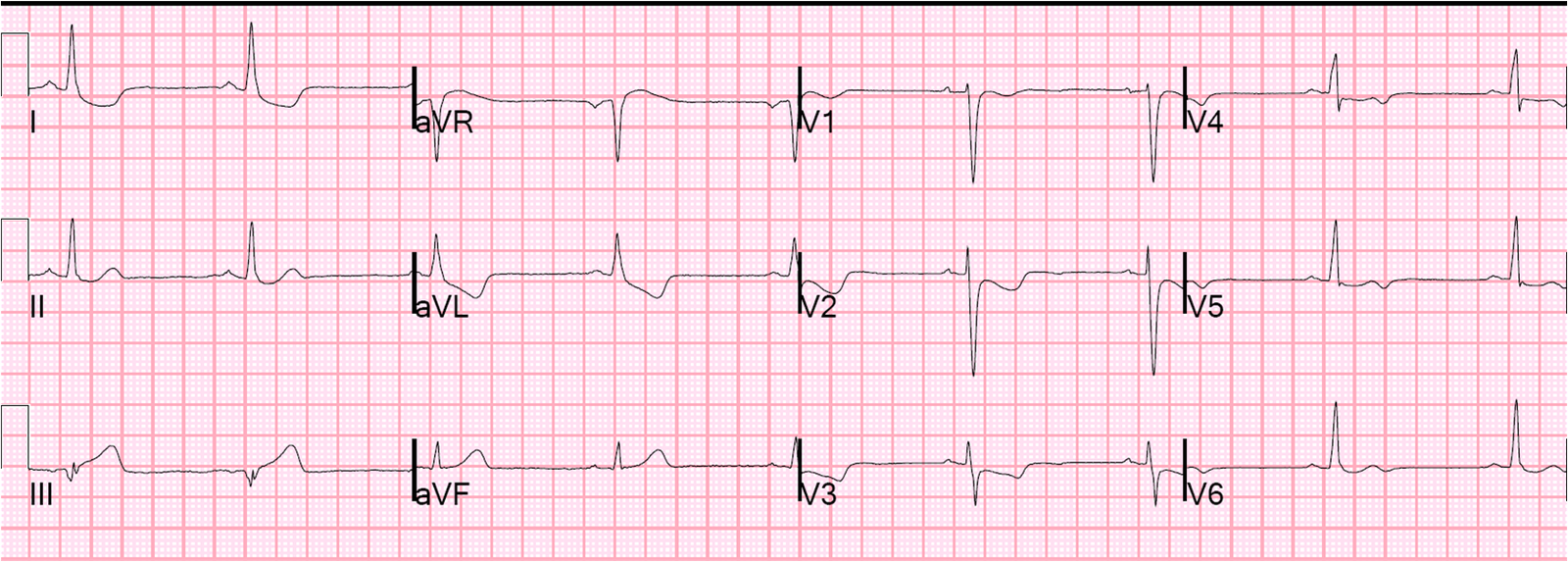
A middle-aged woman with a history of hypertension presented with typical chest pain. Her BP was 160/80. Here was her presenting ECG, with chest pain:
 |
| Inferior leads show hyperacute T-waves and reciprocal STD in aVL, with a reciprocally hyperacute T-wave in aVL. This is all but diagnostic of inferior OMI. There is also subtle STE in V1-V3. In the context of the inferior OMI, this is diagnostic of right ventricular OMI (RVMI). |
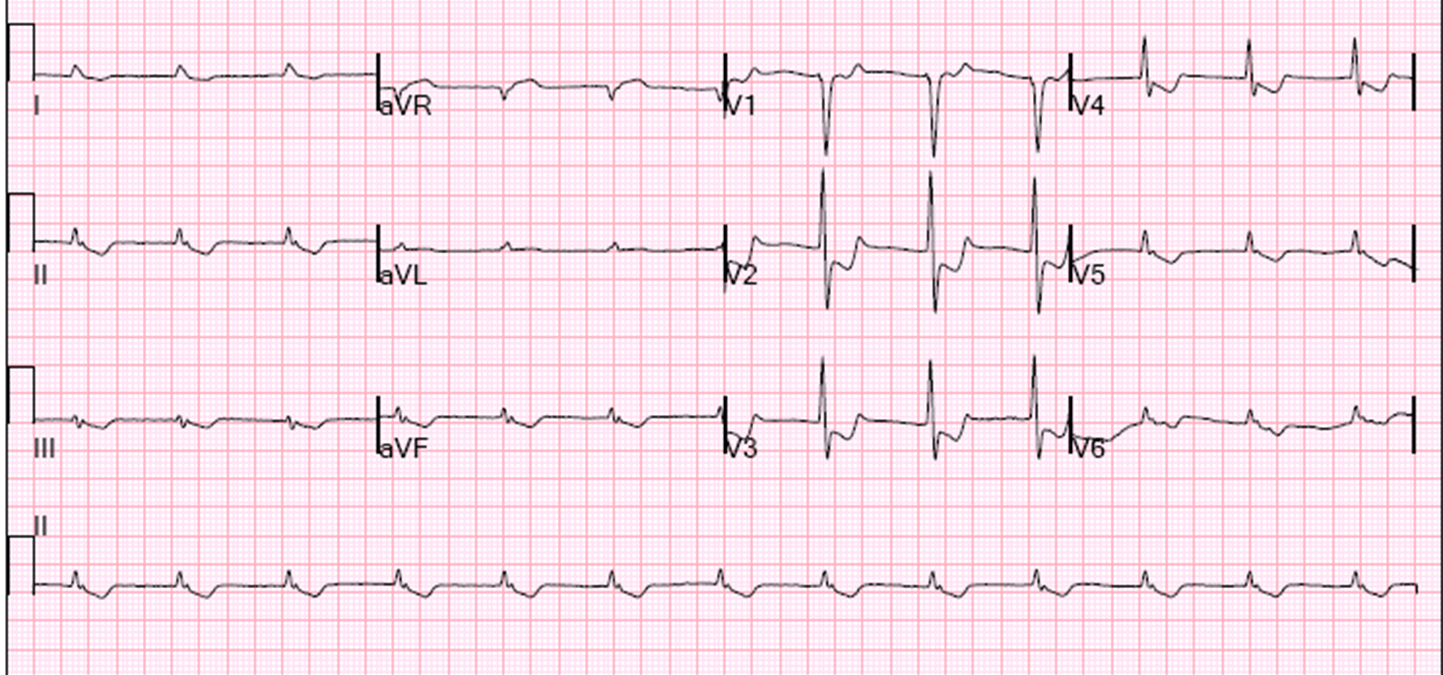
The pain improved with Nitroglycerine. Creatinine was 4.3. She underwent another ECG at 6 hours (when she was pain free):
 |
| The T-waves in leads II, III, and aVF are now significantly smaller, and there is terminal T-wave inversion in III, with reciprocal down-up T-wave in aVL. These are signs of reperfusion. The T-wave in I has also changed. Now these reperfusion findings make the first ECG absolutely diagnostic of OMI |
The troponin peaked at 16 ng/mL (also retrospectively diagnostic of OMI) and there was a “probable” inferior wall motion abnormality.
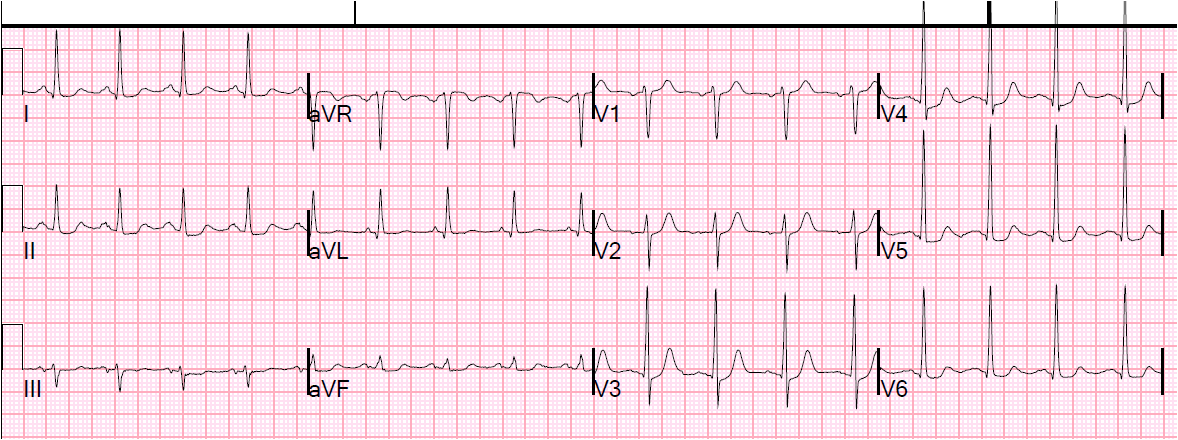
Because the patient had advanced renal insufficiency and because there was “no evidence for a current of injury on her presenting EKG’s”, a non-invasive approach was undertaken. While undergoing a stress test as a part of the non-invasive approach, she developed chest pain and hypotension and had this ECG:
 |
| There is sinus bradycardia with massive inferior ST elevation, as well as ST elevation in V1-V3, diagnostic of inferior and right ventricular (RV) STEMI. When there is ST elevation due to RVMI in V1-V3 in a left sided ECG, it is also called a “Pseudoanteroseptal MI“. |
She went immediately to angiogram and had occlusion of the RCA at the ostium.
Looking back, one can see ST elevation in V1-V3 on the initial ECG that is nonspecific, but, in retrospect, is probably due to RV Injury.