A male in his 60’s with a known history of hypertrophic cardiomyopathy (HOCM) presented for chest pain. He thought it was “acid reflux,” and it started a few hours prior to his presentation to a non-PCI capable hospital. He denied any associated symptoms. His pain was not relieved with NTG. He had an minimally elevated troponin at the referral institution, (assay unknown). He was diaphoretic and clutching his chest. Here is the first ECG:
 |
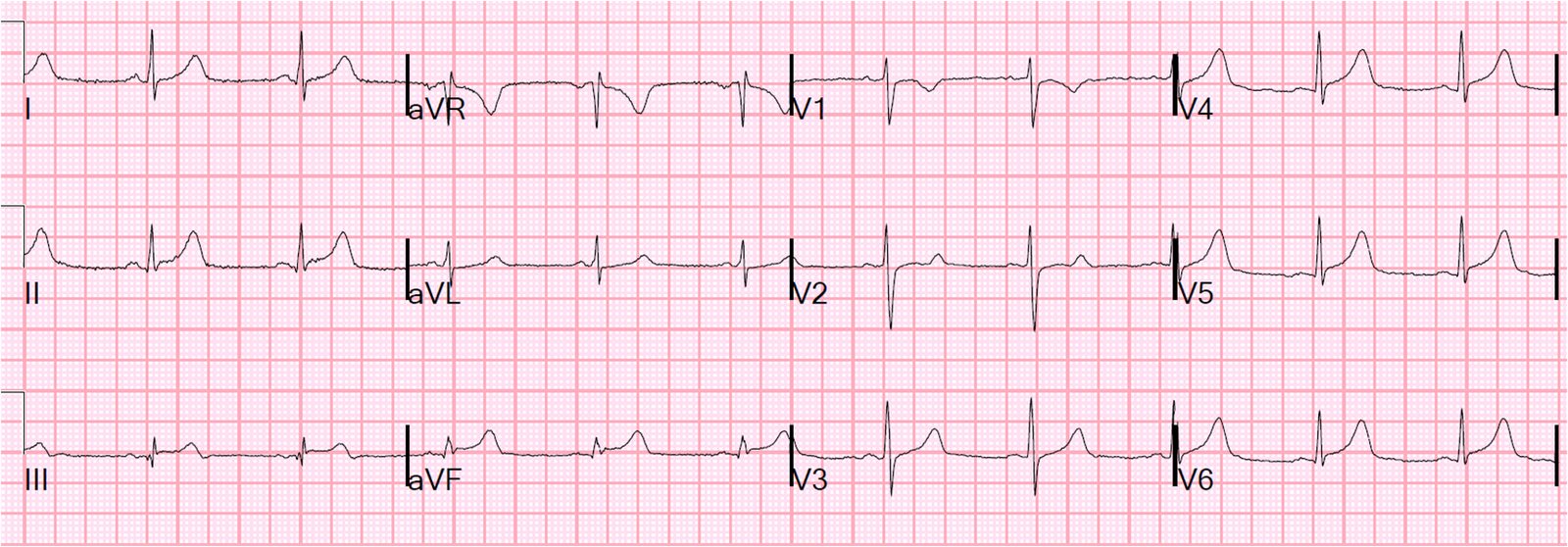
| There is sinus rhythm with LBBB and high voltage, and all leads have appropriate and proportional discordance EXCEPT for lead V4, which has less than 1 mm of (inappropriate) concordant ST elevation. Lead V5 also has significantly less discordance than expected. |
Definitions in Left Bundle Branch Block:
Appropriate Discordance: The ST segment (and usually the T-wave) should be in the opposite direction of the majority (not the end) of the QRS in all leads. It should be proportionate, with the ST/S ratio being < 0.25 or ST/R ratio < 0.30.
Concordance: When the ST segment and/or T-wave is in the same direction as the majority of the QRS. This is abnormal for LBBB and, if 1 mm, a specific sign of STEMI-equivalent.
Any one of:
1. 1 mm of concordant ST elevation in at least one lead. Usually leads I, aVL, V5 and V6. May also involve inferior leads.
2. 1 mm of concordant ST depression in at least one of leads V1-V3.
3. Excessively discordant ST elevation, as measured by ST elevation (at the J-point, relative to the PR segment) to S-wave ratio of > 0.25
What should the ECG look like if there is both HOCM and LBBB? I don’t think anyone knows.
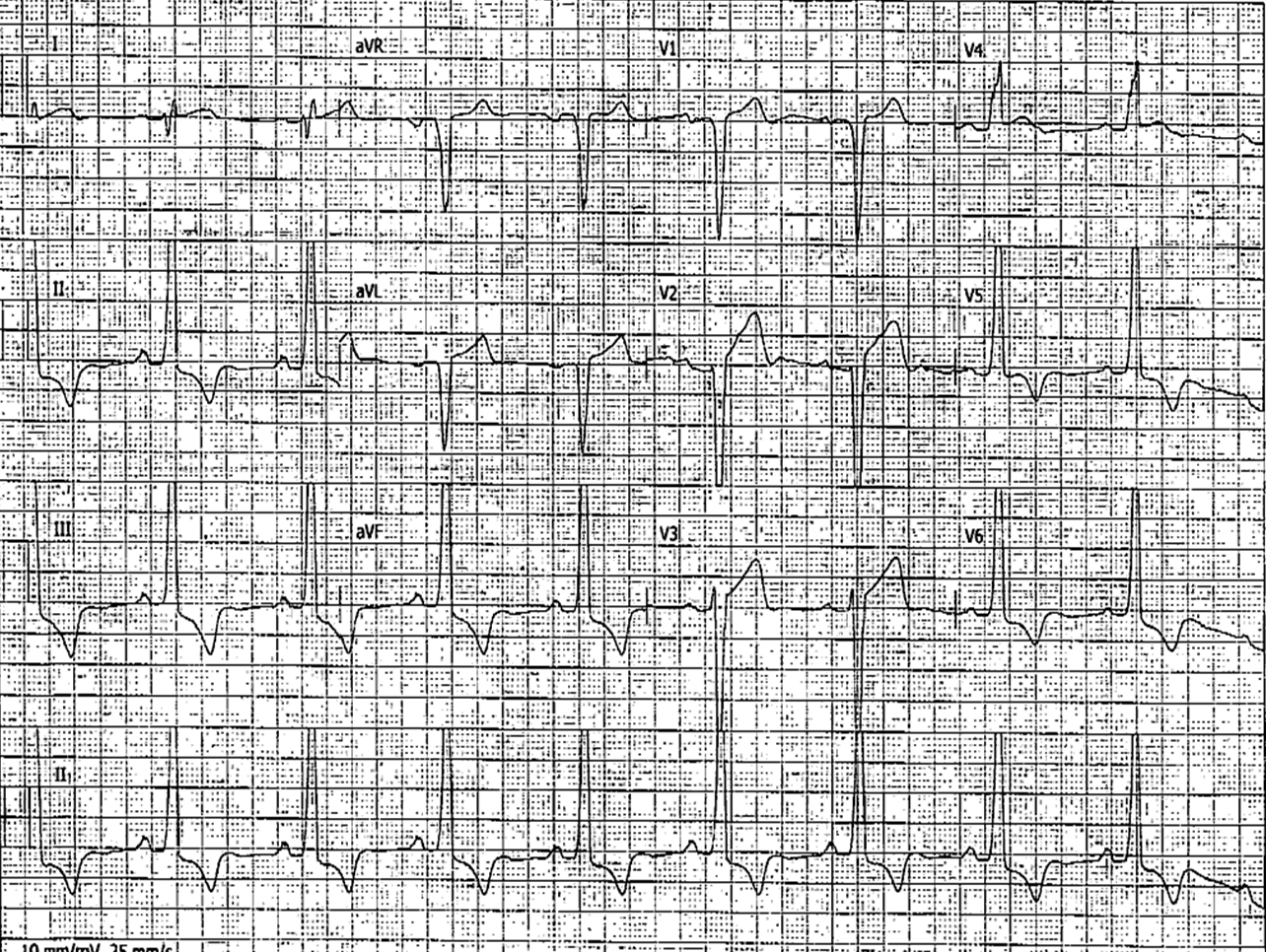
The patient was transferred to a PCI capable hospital where this ECG was recorded:
 |
| Now the concordant ST elevation is in lead V5, but since V4 now has a predominantly negative QRS, the difference is a result of lead placement differences between the two ECGs. V6 has an inappropriately isoelectric ST segment. |
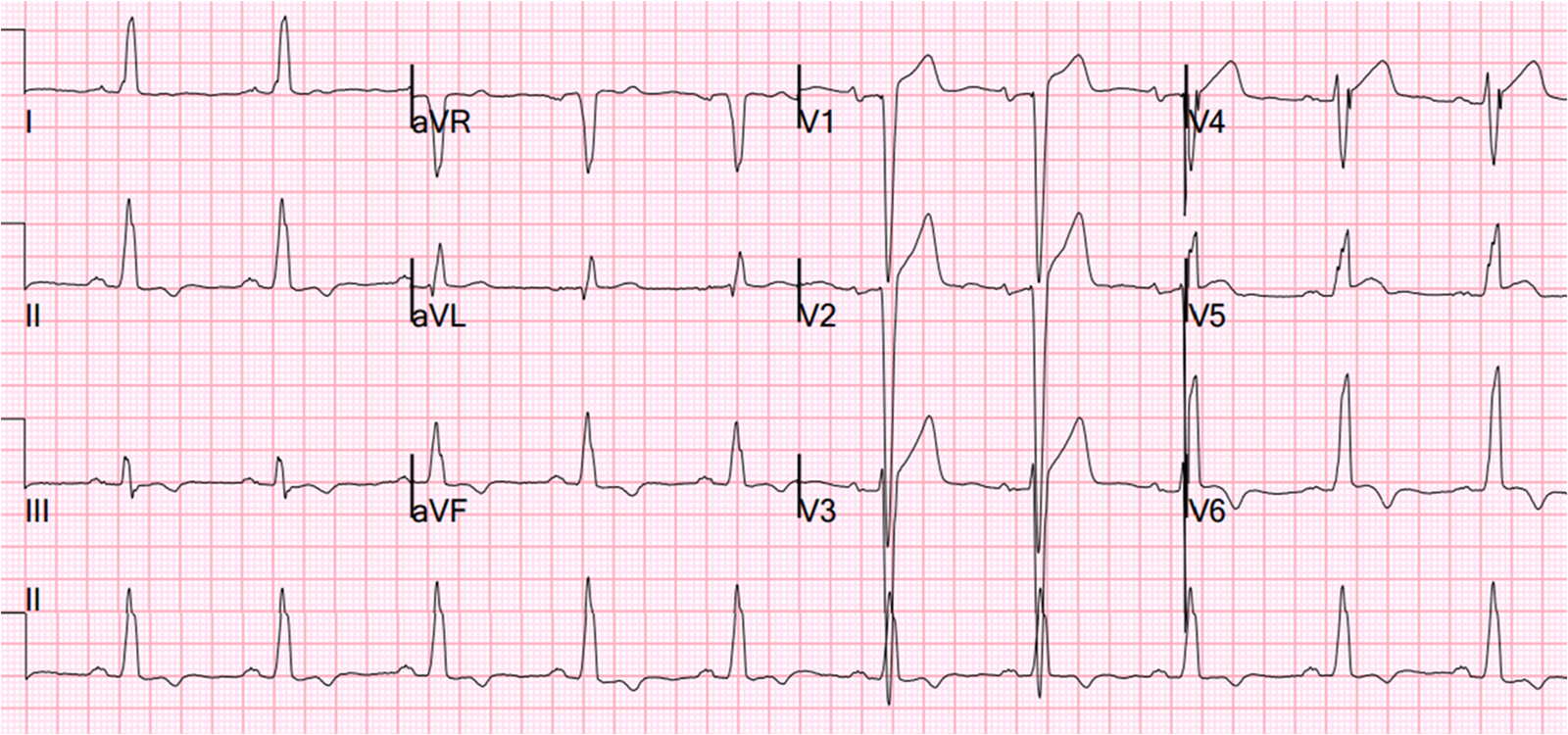
An ECG from 5 years previous was available:
 |
| This shows inappropriate concordance of less than 1 mm in V4, and inappropriate isoelectric ST segments in V5, so all this configuration is not new for this patient who has known HOCM. |
Strictly speaking, none of these meet the first Sgarbossa criterion of 1mm of concordant ST elevation. In our study of patients with ischemic symptoms and LBBB, of 33 occlusions and 129 without occlusion, we had initially hypothesized that ANY concordant ST elevation (not just 1 mm) would be specific for coronary occlusion. We did not publish the data (yet), but less than 1 mm of concordant STE occurred too frequently among the control group to be used as a specific criterion for STEMI-equivalent.
Out of an abundance of caution, the cath lab was activated and the coronaries were clean.
The troponin at the referral institution was normal.
The echocardiogram showed:
Normal estimated left ventricular ejection fraction, about 60%.
Left ventricular hypertrophy concentric, marked.
Dynamic left ventricular outflow/subvalvular obstruction (due to HOCM)
Asynchronous interventricular septal motion due to left bundle branch block.
The outcome
The patient developed abdominal pain in addition to chest pain, had a tender abdomen, and was diagnosed with cholecystitis!!!
Summary
1. Perhaps HOCM in the setting of LBBB can have concordant ST elevation
2. Concordant ST elevation of less than 1 mm has a specificity less than if it is greater than 1 mm
3. Troponins at or near the 99% cutpoint may give discordant results, especially with different assays.