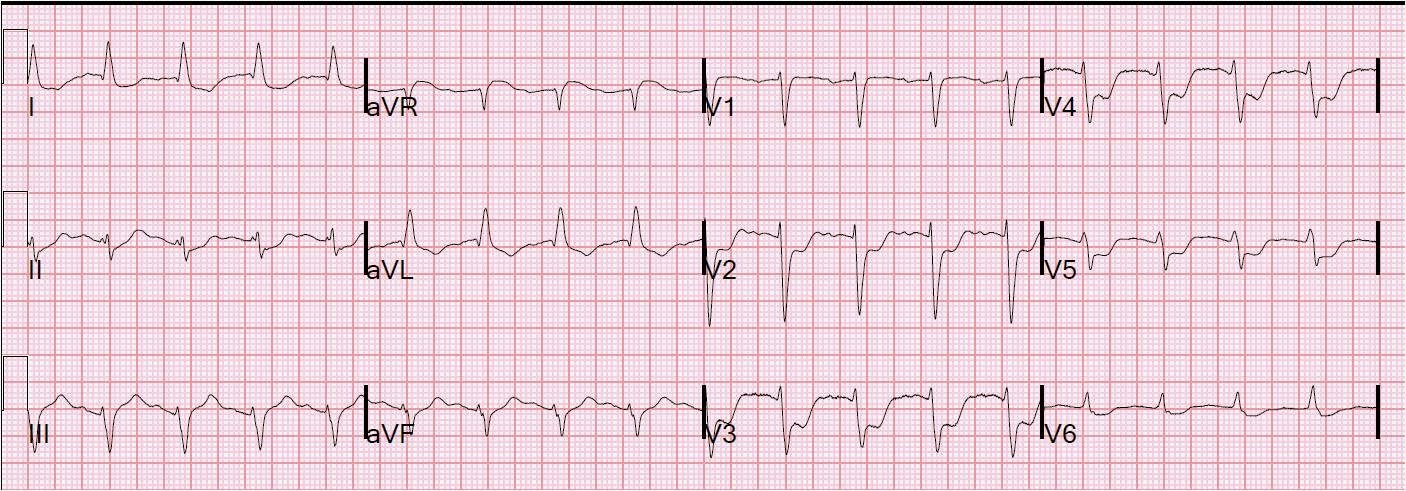
Here is another patient I saw a few weeks ago He is in his 30’s and presented with many hours of chest pain. Here is his initial ECG:
 |
| The computerized QTc is 361. There is ST elevation in V2-V4. Is it normal ST elevation? Normal ST elevation should have good R-waves and V2 and V3 have Q-waves. So this is not normal ST elevation. |
STEMI criteria: 2 consecutive leads with ST elevation, defined as 1 mm in V1 and V4-V6, and, for a 35 year old, 2.5 mm in V2 and V3 (at the J-point relative to the PQ junction). This ECG has at most 1 mm in V2, 1.5-2.0 in V3, and 1.5 in V4, so it does not meet STEMI criteria. LAD occlusion frequently does NOT present as STEMI on the ECG.
With the presence of Q-waves, one should assume this ST elevation is due to LAD occlusion, not to normal variant. Do not even use the formula.
Let’s go back in time
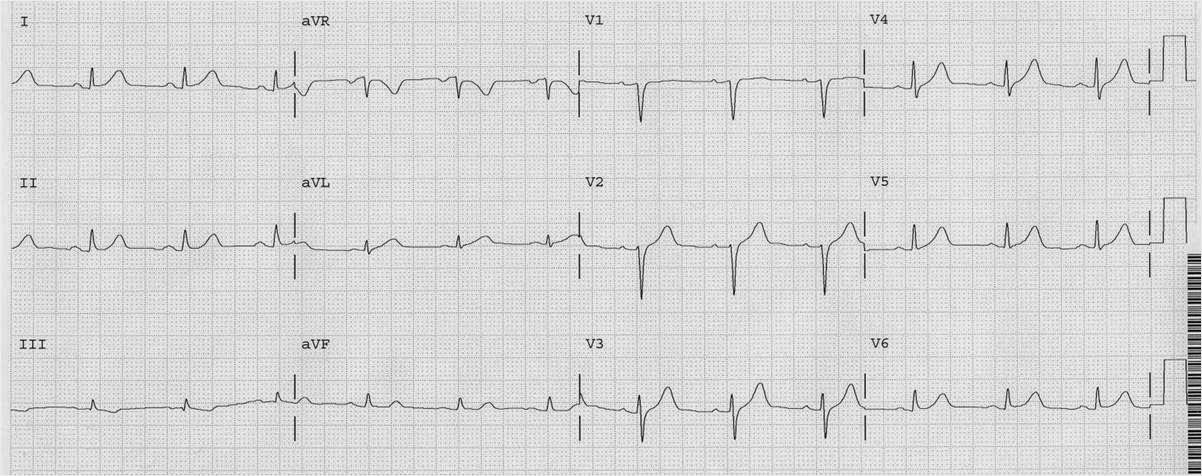
It turns out he had been in the hospital less than a month prior with a NonSTEMI with Wellens’ syndrome. Here is his ED ECG from that visit, after resolution of chest pain:
 |
| Classic Wellens’. Patient is at high risk of closure of his LAD. |
The physicians wanted to do an angiogram, but in spite of pleading with the patient, the patient would not agree to undergo any further testing because he felt fine. They discharged him on aspirin and clopidogrel.
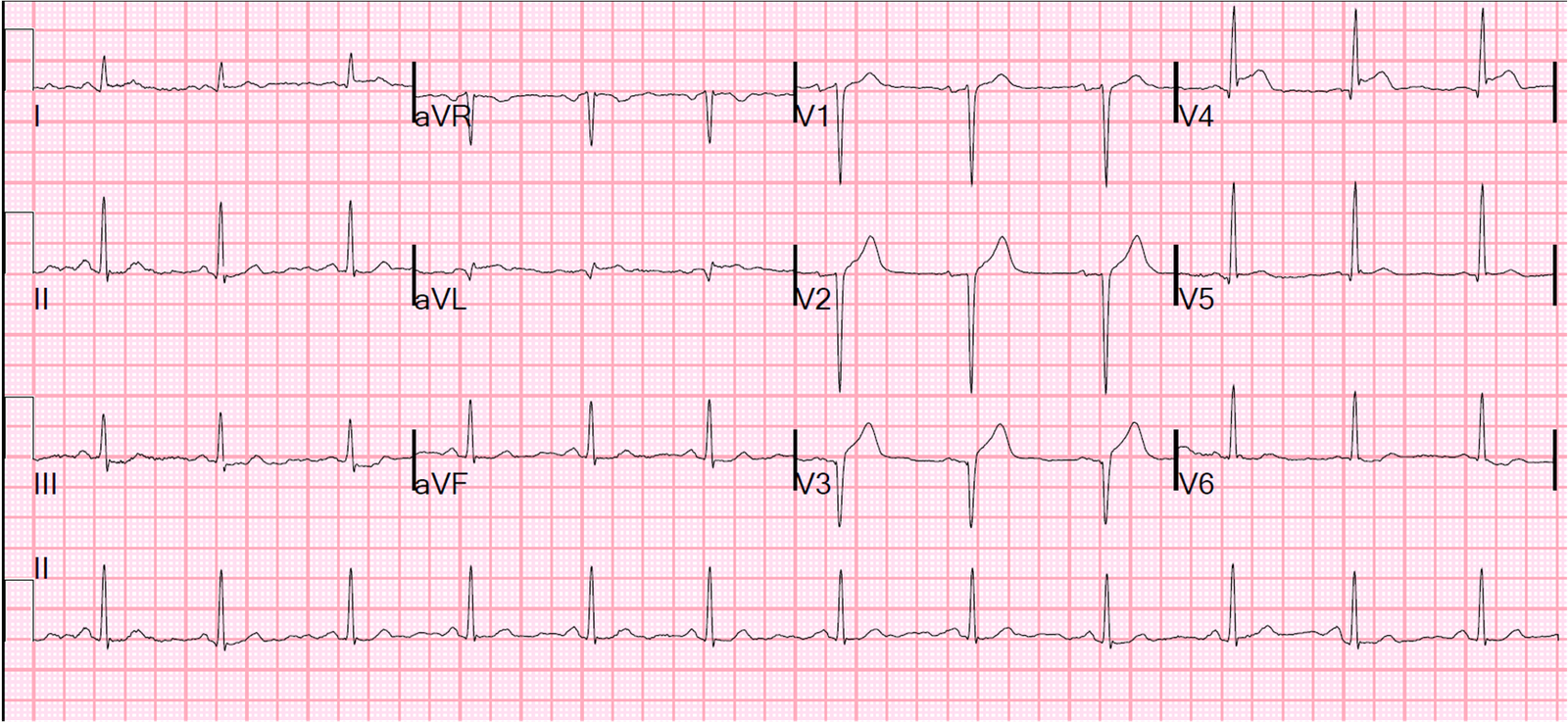
This was his pre-discharge ECG after having a peak troponin I of 0.78 ng/mL (99% = 0.030 ng/mL)
 |
| Notice that much of the T-wave inversion has normalized, but there is residual biphasic T-wave inversion in V4 and V5. |
A pre-discharge echo showed LVH, no wall motion abnormality, and an EF of 60%.
Back to the 2nd ED presentation
And then he presented to me with this ECG, which I post again here so that it is in sequence:
 |
| I did not see this ECG immediately. The computer of course read it as early repolarization. The resident saw it and was worried and ordered a repeat ECG. |
–Had the resident compared with the previous ECG, the loss of R-wave would have made the diagnosis immediately.
–Had the resident seen the pseudonormalization of T-waves (now upright in V4 and V5, all but diagnostic of re-occlusion), the diagnosis would have been made sooner.
–Serial ECGs should not wait an hour
This is ECG #2, 54 minutes after the first:
 |
| Obvious anterior STEMI |
Angiogram showed a proximal subtotal thrombotic occlusion which was stented.
Here is the post cath ECG:
 |
| Marked loss of R-waves with persistent ST elevation. These may resolve over time but are highly correlated with development of LV aneurysm. |
Echo 5 days later showed anterolateral, septal, and apical wall motion abnormalities and an EF of 40%. Peak troponin I was 176 ng/mL (very high).
Learning Points:
1. As I’ve endlessly repeated here, LAD occlusion may be very subtle. Any delay in diagnosis can result in significantly worse outcome.
2. Wellens’ syndrome is the result of reperfusion of a briefly occluded LAD. That LAD is at high risk for re-occlusion
3. Re-occlusion results in pseudonormalization (see link for other cases) of the inverted Wellens’ waves. The apparently normal, upright, T-waves are in fact NOT normal and are the result of re-occlusion.