I saw these two cases on the same day.
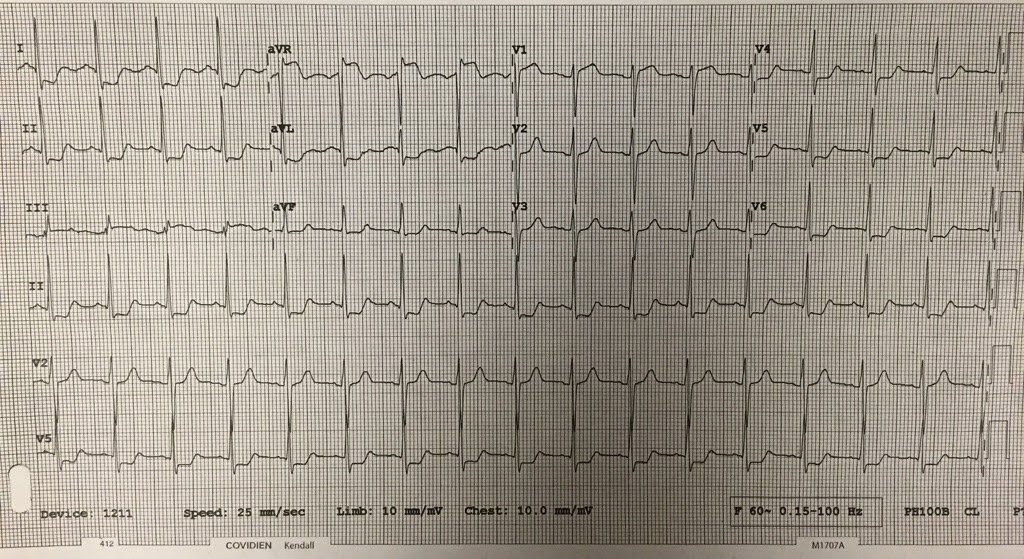
This patient had a GI bleed and a massive transfusion:
| What is it? |
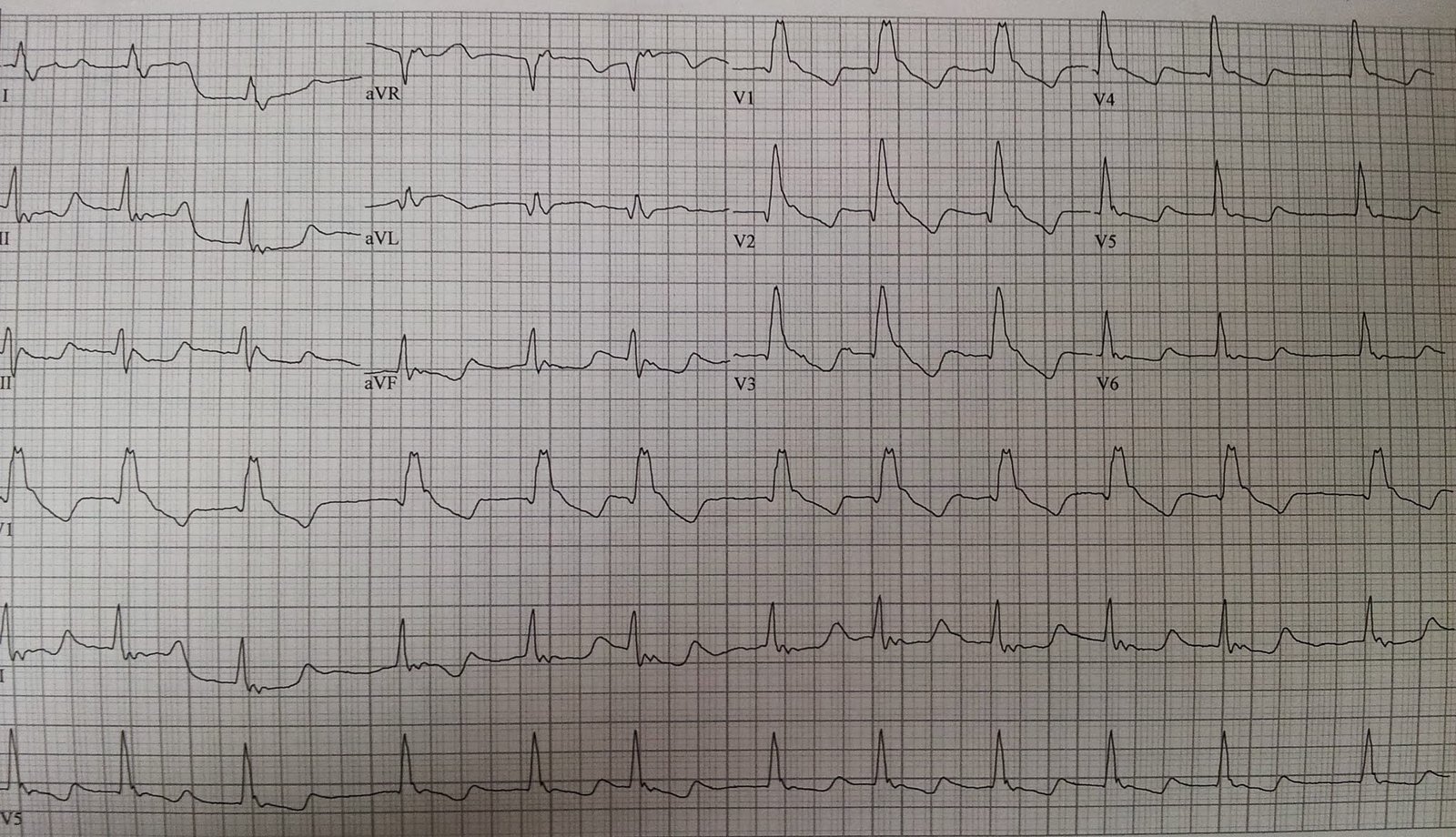
This patient had a history of “frozen shoulders,” and had been treated for this elsewhere for quite a while. He had been seen in the ED 6 days prior for increased shoulder pain, and was referred back to his orthopedic clinic. He had this ECG recorded because shoulder pain can be a symptom of ACS:
 |
| What do you notice? |
The first case has a very long ST segment and thus long QT. This is classic for hypocalcemia; the ionized calcium was 3.0 mEq/L. This is a common complication of massive transfusion. One must be vigilant for hypocalcemia.
The second case shows a very short QT with short ST segment. The computer measured it at 354 ms. This was a tipoff to hypercalcemia and so we suspected that this patient had cancer as the etiology of his pain. A chest x-ray (which we were going to get anyway) confirmed a chest mass. A chest CT confirmed this and also showed otherwise occult spread to the shoulders. The ionized calcium was 7.32 mg/dL and the total calcium was 15 mg/dL.
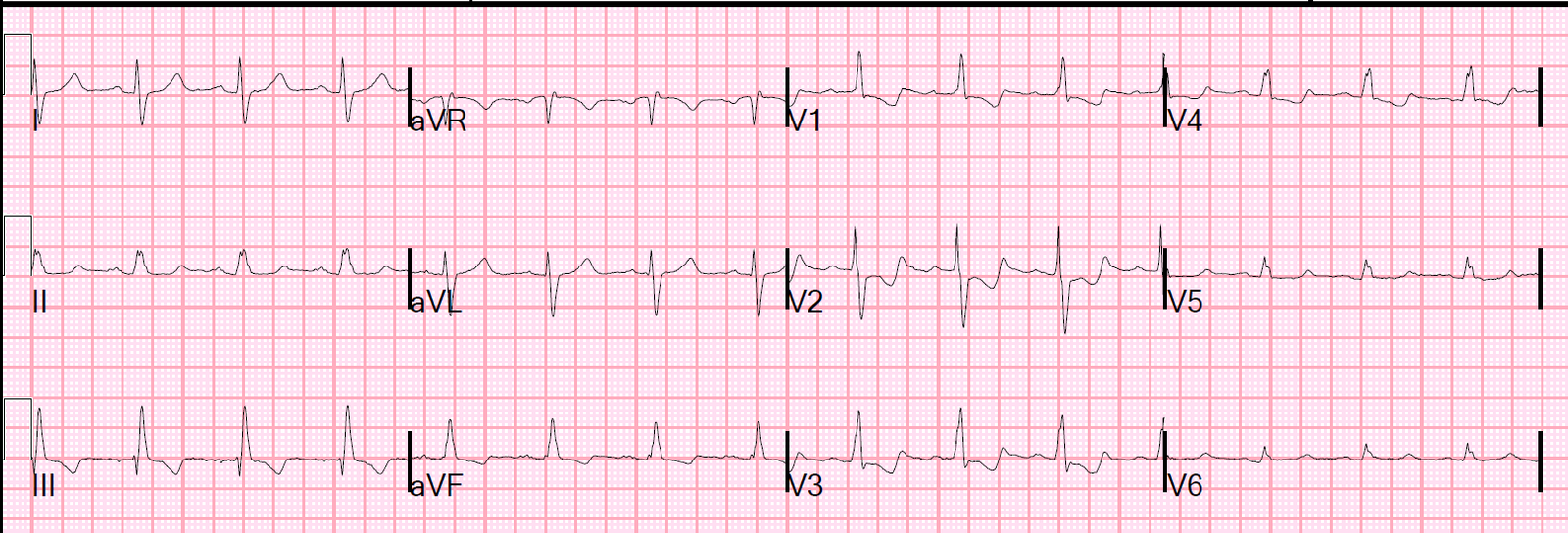
Here was the ECG after normalization of Ca in the second (hypercalcemia) case:
 |
| The QTc is now 384 ms |