This was sent to me, asking what I thought of it:
A very elderly woman presented with weakness and diarrhea. There was no chest pain or dyspnea.
An ECG was recorded because weakness is a common symptom of MI, especially in elderly women.
 |
| What is your interpretation? |
I was told the computer interpretation was “Acute STEMI”.
My response was: “LVH only. No STEMI.”
How do I know?
It is hard for me to explain exactly how I know this except that I have seen it so often and recognize the pattern. But I’ll try.
Features suggesting STEMI:
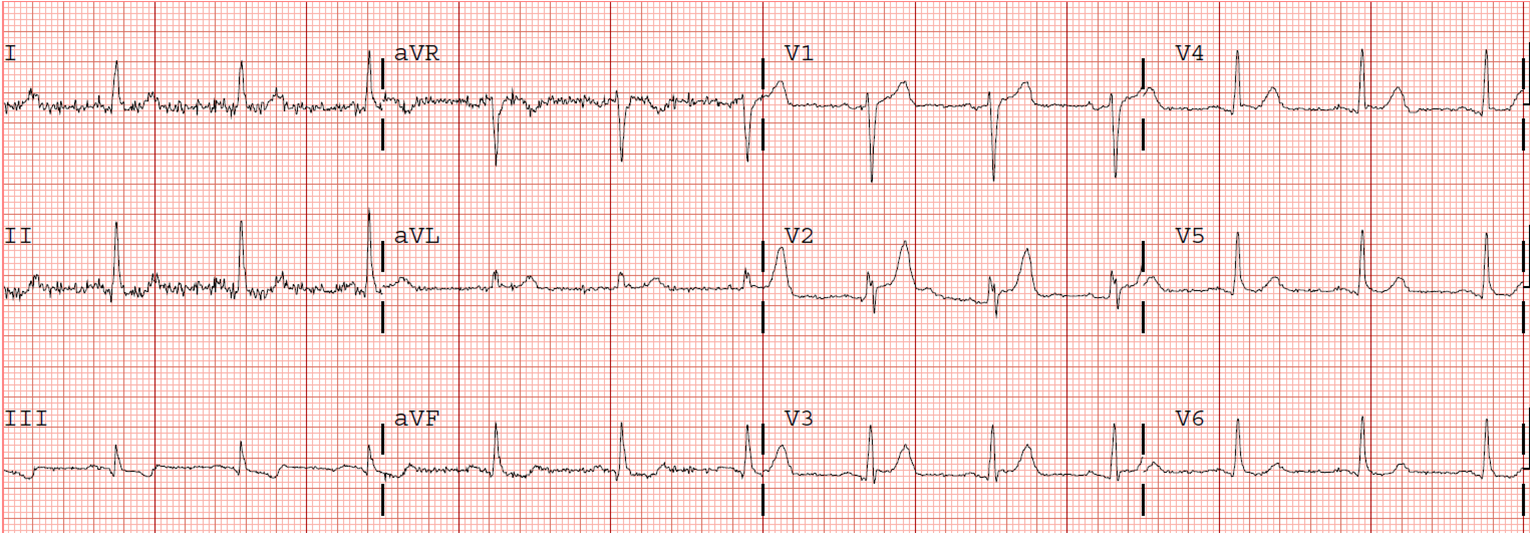
One could easily believe this is inferior-posterior STEMI, as there is ST elevation in lead III with reciprocal ST depression in aVL, and there is ST depression in V2 and V3 with a tall R-wave (the mirror image of a posterior Q-wave).
However:
1. There is high voltage, especially in I, V2, and V3. aVL meets “criteria” for LVH of 11-12 mm amplitude. (As with most ECG features, however, morphology is more important than criteria)
2. The T-wave inversion might be mistaken for NonSTEMI, but then the locations are contradictory: The “inferior” ST elevation would imply active coronary occlusion of the inferior wall, while the T-wave inversion would suggest anterolateral NonSTEMI with reperfusion.
3. The ST elevation in III is not accompanied by any STE in II or aVF. In fact, II has some ST depression. This means that, in the frontal plane, the ST vector is directly to the right at 180 degrees. (In the axial plane it is also posterior, resulting in anterior ST depression)
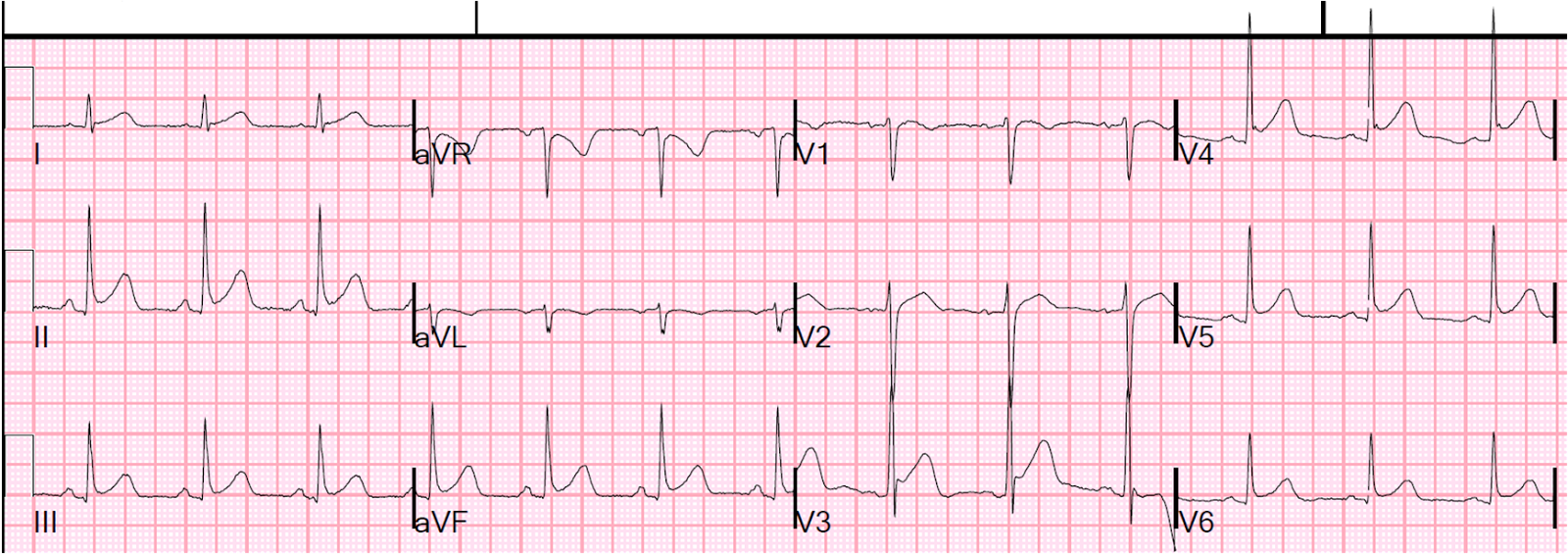
4. ST elevation in III is a scooped-out saddleback, and that is because the ST segment is long and flat, and thus the T-wave is not hyperacute; rather, it has a narrow base. Contrast it with this wide-based T-wave in a true inferior STEMI:
 |
| Lead III
This is STEMI. There is no true saddleback because the T-wave is wide-based (it is particularly fat and bulky resulting in an absence of upward concavity). |
[Although I have found that precordial ST elevation associated with Saddleback is almost never due to MI, I have not assessed it in inferior leads and am not sure of its significance.]
But doesn’t all ST elevation with reciprocal ST depression in aVL mean Acute MI?
No! Absence of ST depression in aVL all but rules out pericarditis and early repolarization as the etiologies of inferior ST elevation. But reciprocal ST depression in aVL is frequently found in these STEMI mimics: LVH, LBBB, inferior LV aneurysm, myocarditis.
Much of ECG interpretation depends on pattern recognition
It is up to those of us who recognize the patterns to figure out what it is that we are seeing so we can communicate it to those who don’t recognize it.
I have long thought that reading ECGs is like recognizing faces (maybe I’m autistic). I have long thought that we need to use computer facial recognition software that can learn from its mistakes, and train it to recognize these patterns.
Fortunately, I have come into contact with some software geniuses who know how to do this and we’re hoping to improve ECG algorithms and make them self-teaching.
The patient did not have an MI.