This case was sent by one of our great FOAM colleagues, Salim Rezaie of REBEL EM!!
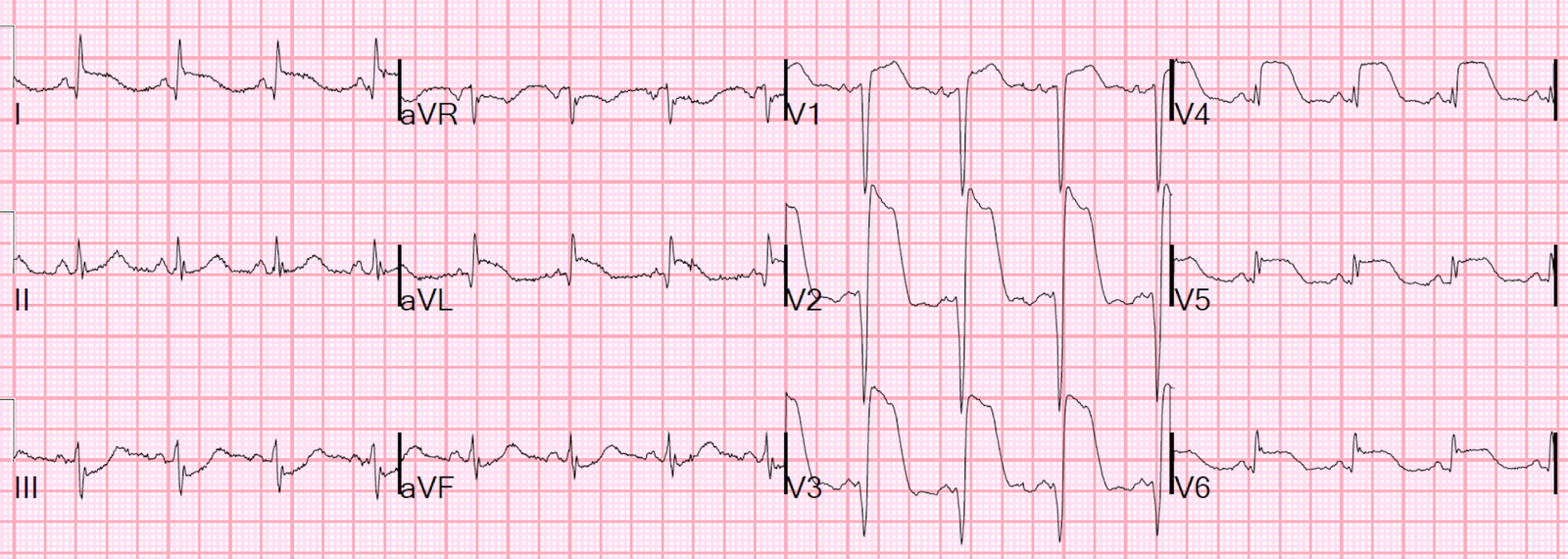
“A 67 y/o female with PMH of Type 2 DM, HTN, Hyperlipidemia, and Hx of MI x 2, with chronic kidney disease awoke at 2am with left sided chest pain. She arrived at 2:45 AM and had this initial ECG below:”
 |
| What do you think? |
Smith response:
There is sinus rhythm. There is No significant ST elevation in any lead. There are large, symmetric T-waves in I, aVL, V2-V5 diagnostic of proximal LAD occlusion. There are also down-up T-waves in III and aVF (these are very specific RECIPROCAL findings and clinch the diagnosis.)
Salim was very worried about these T-waves and so brought the patient the Medical Resus room and did an immediate bedside echo (not shown) which he read as a lateral wall motion abnormality; then he activated the cath lab.
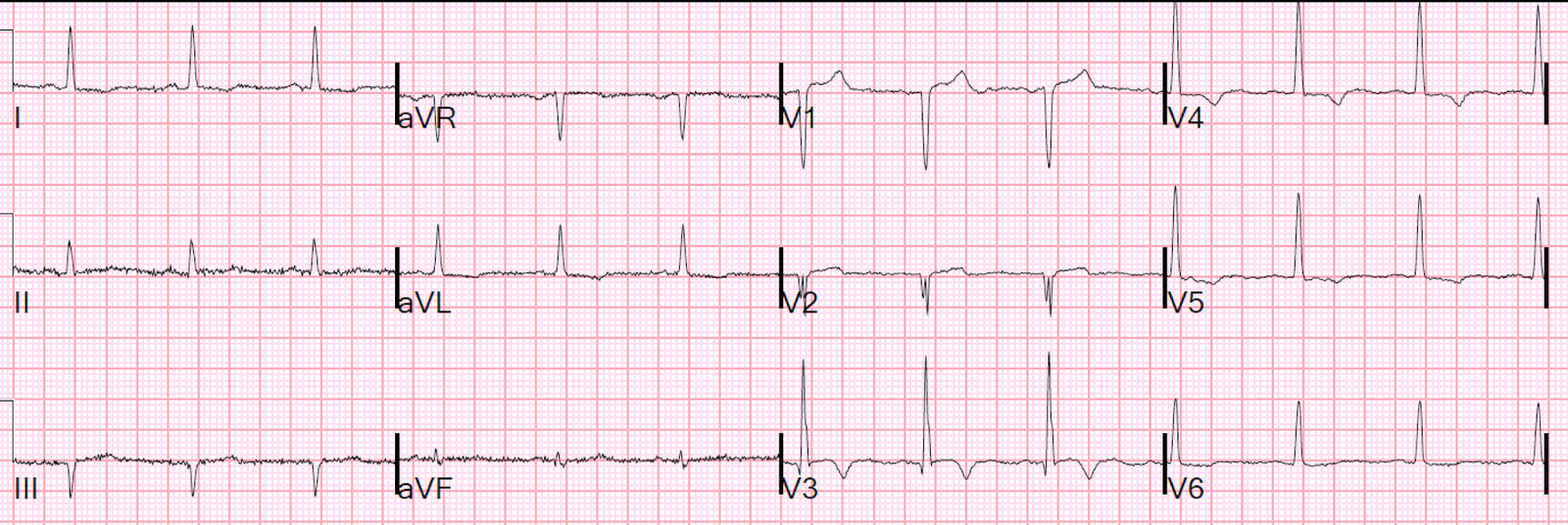
He recorded a second ECG 5 minutes after the first:
 |
| Now there is obvious high lateral ST elevation, as well as STE in V2, V3, V4, V5. |
He writes:
“Patient was immediately taken to cath lab. Initial Troponin was <0 .03="" div="" ml.="" nbsp="" ng="">
(I’m not sure if 0.03 is level of detection or 99% reference, and I did not clarify that with Salim).
“We obtained that result after the patient was already gone. Subsequent Troponin I values were 53.6 ng/mL and 152.04 ng/mL.” This is a large anterior MI.
“In my mind this was a circ lesion due to STE elevation in lateral leads, but….
“Cath showed:
“Prox LAD 70% lesion
Large D1 100% occlusion
Distal LAD old 100% occlusion
Proximal Circ 20%
Prox RCA 50%”
“The reason I found this case interesting was two reasons:
“1. Initial ECG did not quite meet STEMI criteria, but obviously very concerning t waves and bedside echo findings.
“2. STE in 2nd ECG seen in lateral leads but also V2, V3, V4. Looks like reading in the literature you can have STE in aVL and V2 and this is commonly described with D1 lesions not circumflex lesions.
“Interested in your thoughts and if you think it is worthwhile for a Dr. Steve Smith blog post. Hope you are well.”
Salim
My thoughts?:
Great Case and Great job diagnosing this subtle LAD occlusion and getting her to the cath lab fast!
Culprit artery comment
STE in aVL and V2 does indeed often occur with a D1 lesion. Some call it a “mid anterior MI“. In this case, though, as you say, the T-waves (EKG 1) and STE (EKG 2) were out to V5 and even V6, so this is the territory of a proximal LAD but still could be a D1 that serves a very large territory.
If there was thrombus, the proximal LAD 70% may have been occluded at the time of the EKG and this would account for all findings. A co-culprit in D1 would not be terribly unusual.
Circ lesions with STE in aVL: if they have any precordial finding, it is usually ST depression in V2 and V3 (simultaneous posterior MI), whereas D1 lesions look like this.
Overall Impression
The first ECG is immediately diagnostic to my eye, perhaps partly because the image from this case is burned into my retina:
35 yo woman with LAD occlusion manifesting with only hyperacute Ts and inferior ST depression, also missed by computer