A late middle-aged male with h/o 3 vessel bypass (CABG), type 2 diabetes, peripheral vascular disease, DVT, Chronic Kideny Disease, and chronic combined systolic and diastolic congestive heart failure presented with chest pain which started approximately 2 hours prior to arrival.
Here was the initial ED ECG:
 |
| Sinus Rhythm
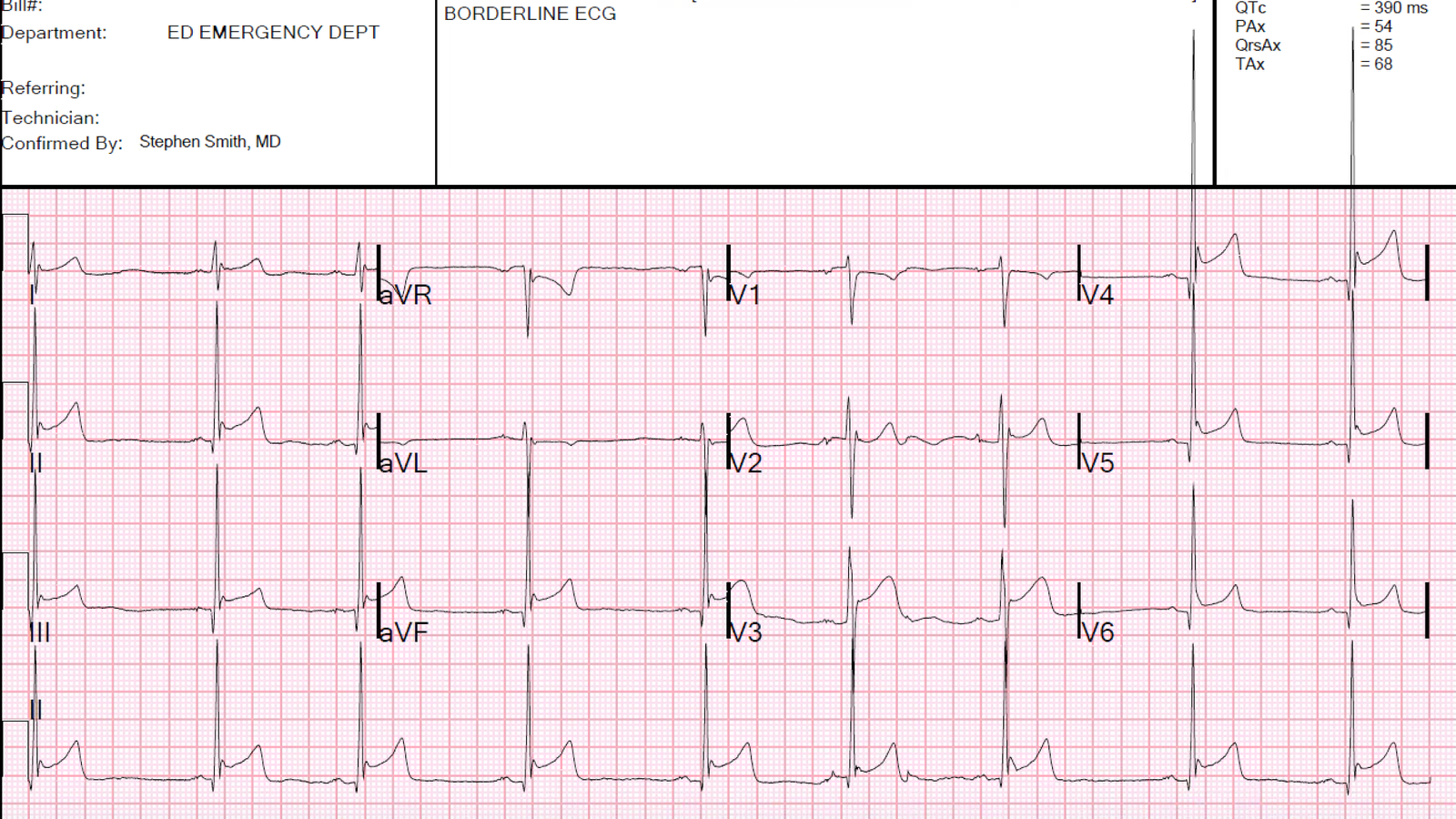
There is an rSR’ in V1, with wide S-waves in lateral leads (right bundle branch block, RBBB). Normally, RBBB has a bit of ST depression in V1-V3 that is discordant (in the opposite direction of) the R’-wave. So that bit of ST Depression in V1 is normal. What about V2 and V3? |
Notice there is no R’-wave in V2 and V3!! This happens in some RBBB when there is very early transition. Normally, in RBBB, there is indeed an R’-wave in V1-V3. Here it is only in V1, and the wide S-wave which is normally seen in V4-V6 starts all the way rightward at V2. Therefore, one should not expect any ST depression in V2.
But this was made easier because there was a previous ECG available:
 |
| There is no ST depression in V2 and V3 on this old ECG Also, there was no STD in V1 either |
No action was taken, but a second ECG (below) was recorded 80 minutes after the first. In the meantime, a nitro drip had been started and aspirin and heparin given.
This one was texted to me with the words: “Ongoing improving pain with trop 0.13 (elevated). Creatinine 2.2.”
T=80 minutes:
 |
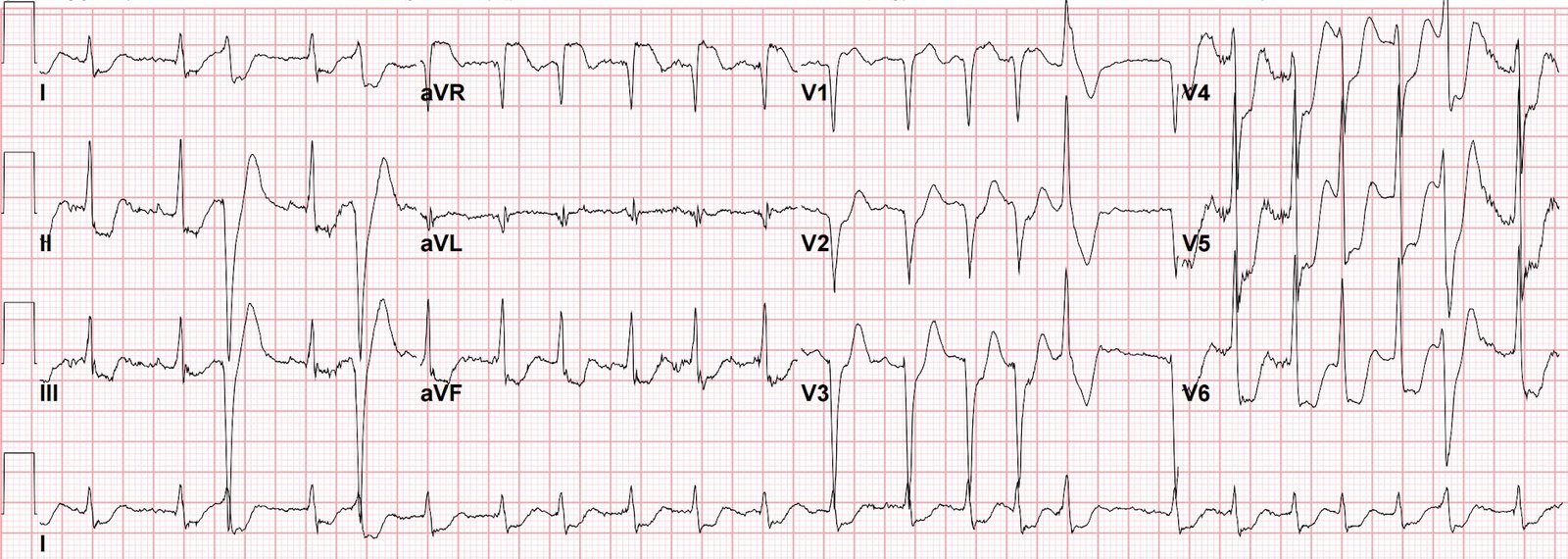
| I could only see it on my phone, and I had no other clinical info. I responded: “An unusual RBBB, but there is quite a bit of ST depression in V2 and V3. Must assume it is ischemic. Must go to cath lab unless it resolves” When I had a chance to view these on a full screen, it became clear that this is all but diagnostic of posterior STEMI. Not all ST depression in V2 and V3 is posterior STEMI, but it is posterior STEMI until proven otherwise. Note: posterior leads do not help here: no matter what the cause of the ST depression in V2 and V3, the posterior leads will reflect the opposite! This is an electrical necessity! They will not be able to determine the cause of the ST shift. It is well known that the most likely cause is posterior STEMI. |
When should you record posterior leads? If you suspect ischemia and it is not showing on the 12-lead, on occasion it will manifest in posterior leads only.
The patient’s pain completely resolved on a nitro drip.
He was admitted.
There was a 3rd ECG at 240 minutes:
 |
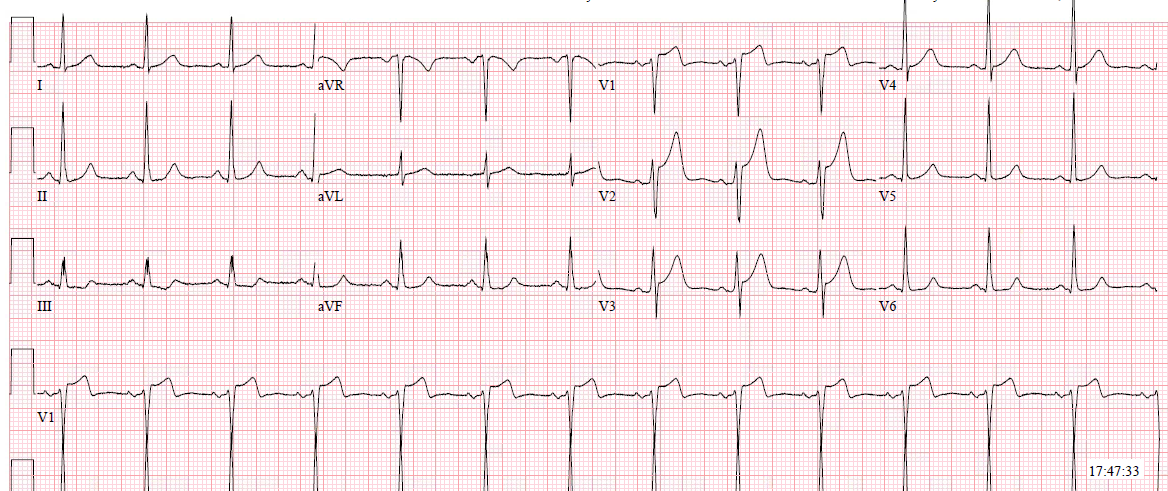
| ST depression is mostly resolved, but the ECG has not returned to baseline. |
A 4th ECG was recorded at 360 minutes:
 |
| No difference from 240 minutes |
The patient had positive troponins and was scheduled for angiography to begin about 16 hours after arrival in the ED.
Complication: While waiting in the cath lab prep room, he had VT and V Fib arrest.
Fortunately, he was easily defibrillated.
Here is the 12-lead recorded immediately after resuscitation:
 |
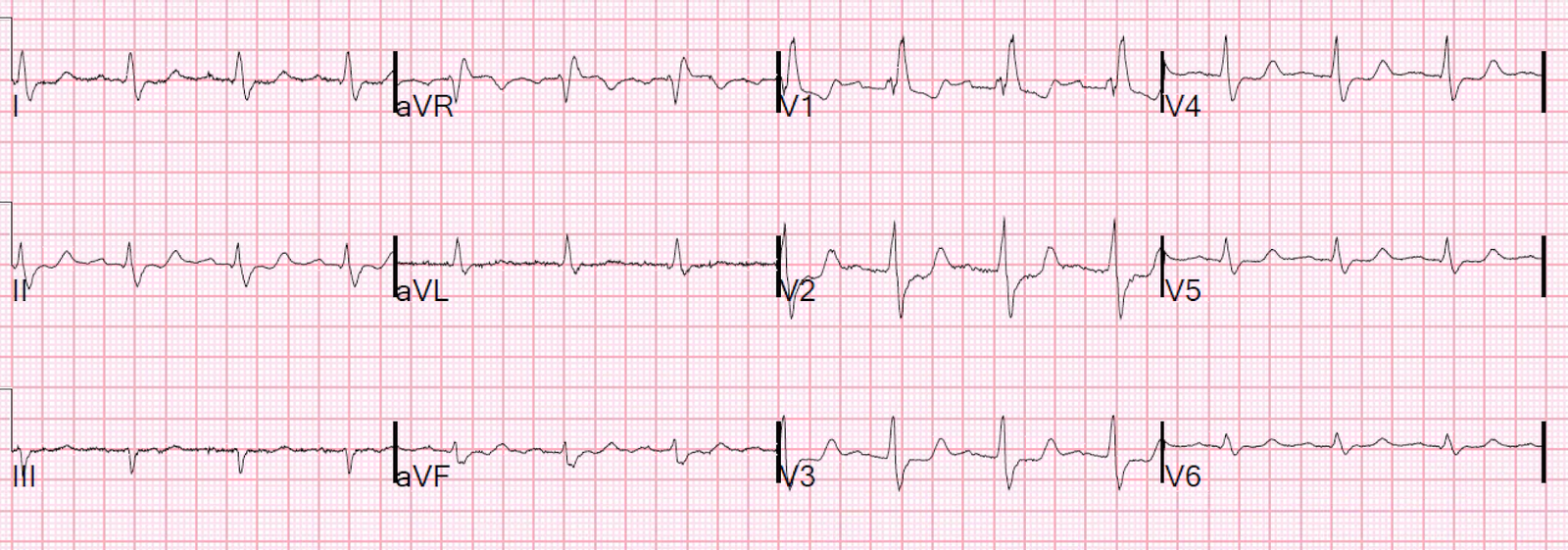
| There is sinus bradycardia with a junctional escape. RBBB persists Now there is profound ST depression in V1 and V2 |
Angiogram: it is complex because of previous CABG, but the bottom line was that there was an acute 99% thrombotic occlusion of the saphenous vein graft to the obtuse marginal (to the posterior wall).
Echo: Dyskinesis of the basal to mid inferior and inferolateral segments. (Basal inferior segment is equivalent to the posterior wall). EF 45% (not significantly changed from prior).
Peak troponin I: only 2.94 ng/mL.
The patient did well. Here are subsequent ECGs:
Immediate post cath ECG:
 |
| There is trigeminy: complexes 2, 5, 8, and 11 are all PVCs (each is in the middle of the 3 complexes in each of (I, II, III / aVR, aVL, aVF / V1-V3/ V4-V6).
ST depression is mostly resolved. |
ECG at 36 hours:
 |
| Some persistent ST depression. |
ECG at 60 hours:
 |
| All ST depression has resolved. |
Summary
The patient was fortunate to have a STEMI with delayed treatment that did not result in a lot of myocardial loss.
Final formal diagnosis: NonSTEMI
You can see what a misnomer this is. It is a STEMI, but with failure to record ST elevation because the 12-lead does not record over the posterior wall.
This is therefore another example of the False STEMI-NonSTEMI Dichotomy
See my lecture on this topic:
Lecture at the 2015 SMACC Chicago conference:“The False STEMI-NonSTEMI Dichotomy”.
Learning Points
1. Ischemic ST depression in V2 and V3 due to ACS is posterior STEMI until proven otherwise.
2. It should be called STEMI
3. RBBB has up to 1mm of normal ST depression in V1-V3, but ONLY when there is an R’-wave!! That ST depression is rarely more than 1 mm (and then only when the R’-wave is very large, such as in right ventricular hypertrophy)
4. If you treat a patient with a “NonSTEMI” medically, with delayed cath lab, you MUST monitor extremely closely. Arrest can happen at any time.