A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chest pain.
Here is the EMS ECG:
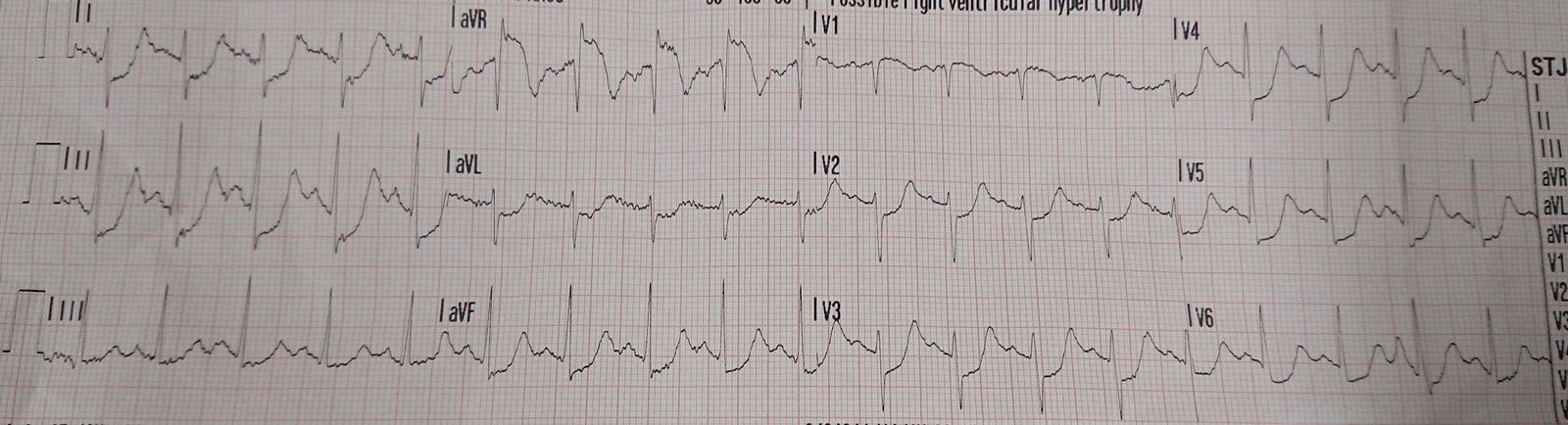 |
| Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR
Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. |
EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chest pain from an 8/10 to 4/10.
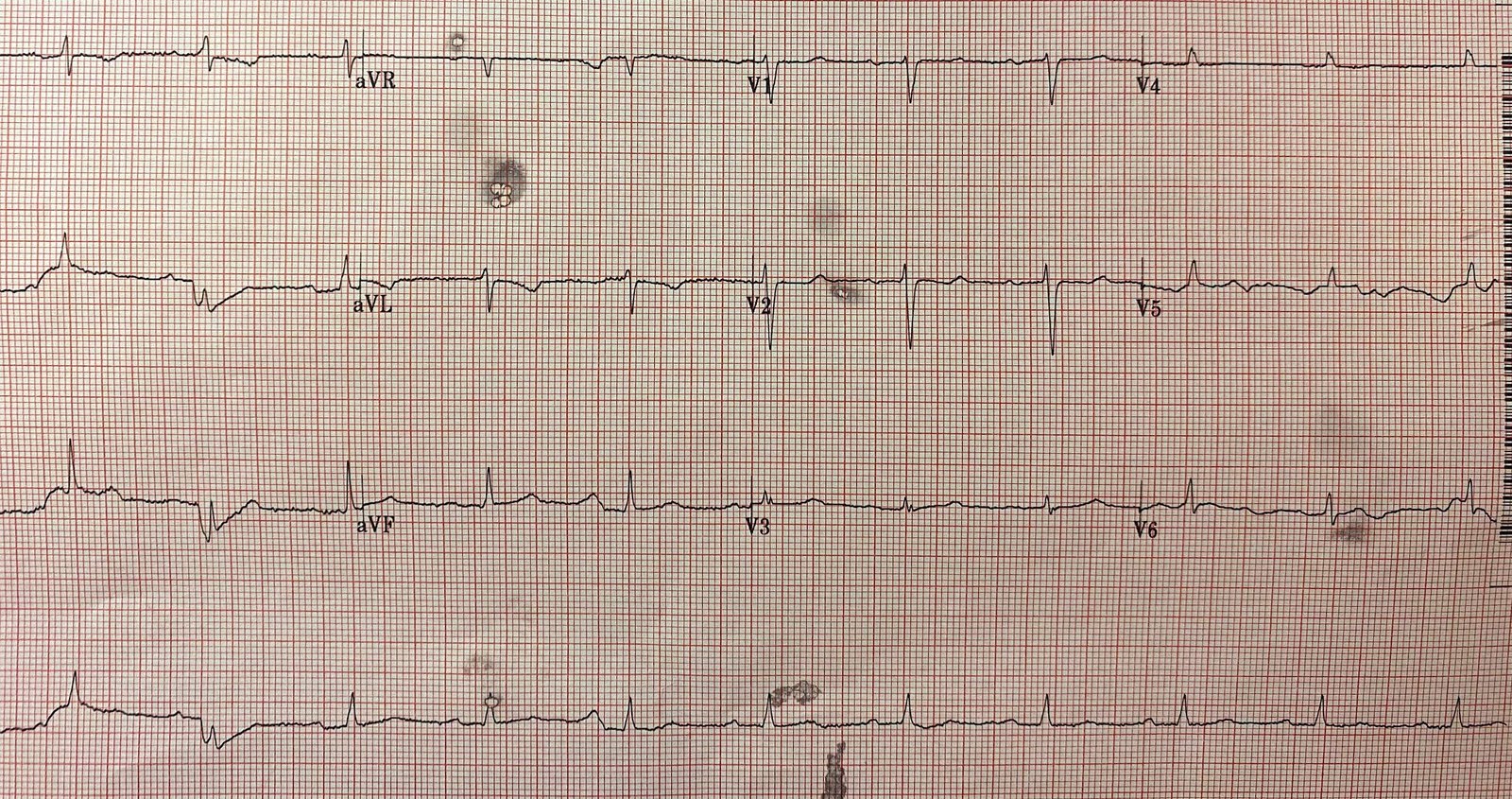
Here is the ED ECG on arrival:
 |
| Less STE/STD |
Provider’s Clinical Impression: “findings concerning for myocardial infarction, likely proximal LAD or Left main.”
Cath lab activated
Dual antiplatelet therapy and heparin given. NTG drip started. Pain better still.
What do you think the echocardiogram shows?
First trop I returns at 1.5.
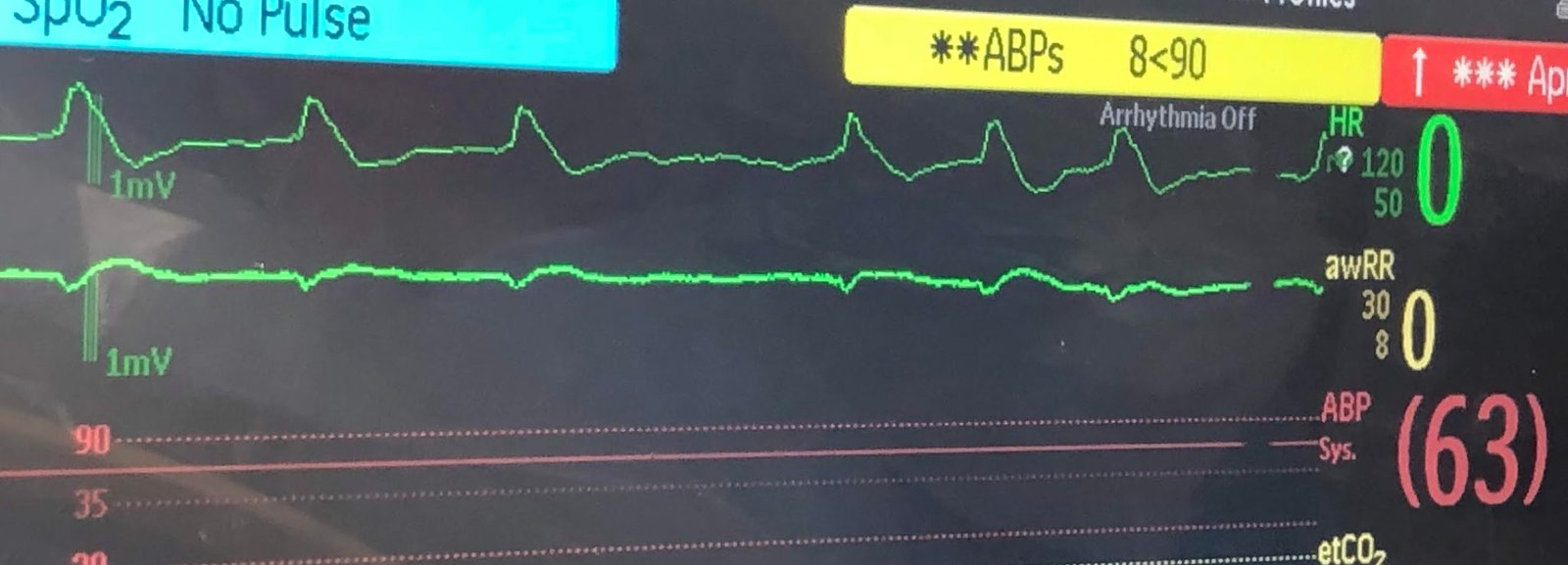
POCUS Echo:
POCUS Echo with no wall motion abnormality and normal ejection fraction.
This was a point of care ultrasound, not a bubble contrast echo. Sensitivity of POCUS even for definite wall motion abnormalities is far from perfect.
But there are frequently no wall motion abnormalities when there is diffuse subendocardial ischemia. This is an anecdotal observation that I and others I know have made, and I cannot find any formal literature on the topic. I have posted previous such cases, but in searching my own blog, I could not find them.
It would be a good topic for study.
Angiogram:
Severe diffuse left main disease, up to 80% at the ostial left main. Stented.
Post cath ECG:
 |
| Normal or near normal |
Peak troponin I was 15 ng/mL.
The post cath contrast echo also showed no Regional wall motion abnormality. One would not expect wall motion to recover so quickly after stenting, so this is good evidence that the POCUS echo was indeed accurate.
Why would there be no Regional wall motion abnormality?
It is because the epicardium remains functional; it is only the endocardium that is ischemic, and it is ischemic everywhere. So both are true: no decrease in EF and no WMA.
Is this OMI? Not strictly speaking, but cath lab activation is usually required.
There is a subtle but important difference between OMI and subendocardial ischemia: OMI (that is not STEMI) is due to TIMI 0/1 flow and has any combination of subtle STE, hyperacute T-waves, reciprocal ST depression, decreased QRS amplitude, terminal QRS distortion and other findings. It is distinguised from subendocardial ischemia (SI) in that SI has diffuse ST depression with reciprocal ST Elevation in aVR. The artery is open, but flow is insufficient to perfuse the entire myocardial thickness (subendocardial AND subepicardial).
On echo, OMI has a wall motion abnormality, but SI usually does not.
![]()
===================================
MY Comment by KEN GRAUER, MD (5/13/2020):
===================================
It’s good to periodically review the differential diagnosis of the diffuse subendocardial ischemia. Recognition of this ECG pattern should be an automatic REFLEX for the emergency care provider — As soon as one sees diffuse ST segment depression (usually present in at least 7-8 leads) + ST elevation in lead aVR — one should consider:
- Severe Coronary Disease (due to LMain, proximal LAD, and/or severe 2- or 3-vessel disease) — which in the right clinical context may indicate ACS (Acute Coronary Syndrome).
- Subendocardial Ischemia from another Cause (ie, sustained tachyarrhythmia; shock/profound hypotension; GI bleeding; anemia; etc.).
The initial tracing in this case illustrates an extreme example of this phenomenon — in which all leads except for aVR and V1 manifest profound ST segment depression (Figure-1).
- ST depression attains up to 5 mm in several leads!
- A comparable amount of reciprocal ST elevation is seen in lead aVR.
- As is seen in ECG #1 — a lesser amount of ST elevation is sometimes seen in lead V1.
 |
| Figure-1: The initial ECG in this case, done in the field by the EMS team (See text). |
In the March 9, 2020 post of Dr. Smith’s ECG Blog — Dr. Smith presented results from a 2019 article by Harhash et al, that confirm how the ECG pattern shown in Figure-1 does not represent acute LMain occlusion — but rather the differential diagnosis that I show above.
- The case I presented in My Comment to that March 9, 2020 post showed a patient with this pattern — who on cath had no more than minimal coronary disease.
- Dr. Smith also referenced an article by Knotts et al, showing that even when diffuse subendocardial ischemia is due to coronary disease — that only a minority of patients had severe LMain coronary disease as the cause.
Today’s Post by Dr. Smith adds to our knowledge of this syndrome. For as helpful as POCUS Echo can be in the diagnosis of acute coronary occlusion — we need to remember that there are frequently no wall motion abnormalities when there is diffuse subendocardial ischemia — because (as emphasized by Dr. Smith): i) The epicardium remains functional, since it is only the endocardium that is ischemic; and, ii) Subendocardial ischemia is diffuse — and therefore does not localize to any particular myocardial region.
P.S.: Much of the time — the amount of ST depression (and the amount of reciprocal ST elevation in lead aVR) will not be as extreme as it is in Figure-1. Nevertheless, this ECG pattern of subendocardial ischemia needs to be instantly recognized — so that optimal decision-making based on the clinical scenario can promptly begin (See the October 31, 2018 post on Dr. Smith’s Blog).
![]()