A 60-something male presented with 2 hours of chest pain.
Here is his ECG:
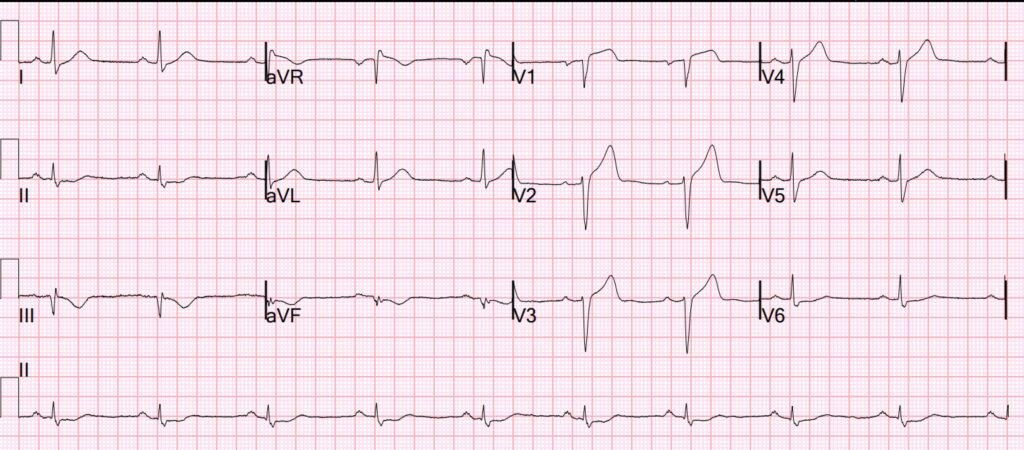
What do you think?
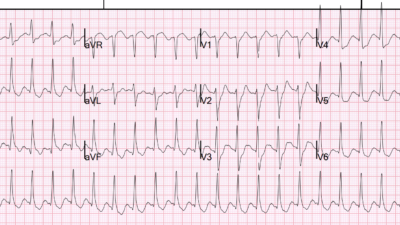
This is diagnostic of proximal LAD Occlusion (LAD OMI). There is STE and Hyperacute T-wave (HATW) in V1, HATW in V2-V4 (with some STE), STD in V6 (thus, making for precordial swirl pattern). There is a reciprocally inverted T-wave in lead III, and reciprocal STD in II and aVF.
Precordial swirl usually represents occlusion proximal to the septal artery, causing septal transmural ischemia. V1 sits right over the right side of the septum and manifests STE and HATW. V6 is opposite
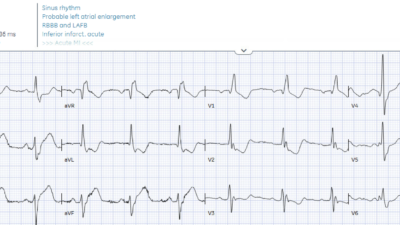
Here is the conventional algorithm interpretation (Veritas algorithm):
–SINUS BRADYCARDIA
–INFERIOR MYOCARDIAL INFARCTION , OF INDETERMINATE AGE [40+ ms Q WAVE AND/OR ST/T ABNORMALITY IN II/aVF]
–ABNORMAL ECG
Part of the reason that the algorithm does not diagnose STEMI (and will never diagnose OMI) is because the ECG does not meet STEMI millimeter criteria. There is > 1 mm STE in lead V1 but only 1.5 mm in V2 and less in the other leads.
Here is the PMCardio Queen of Hearts AI ECG Model interpretation:

The very astute ED team immediately recognized OMI and activated the cath lab.
There was a total Proximal LAD Occlusion which was opened and stented.
= = =
==================================
MY Comment, by KEN GRAUER, MD (6/15/2026):
If you wanted to quickly determine how skillful a clinician is at recognizing acute OMIs — You could do so by using today’s case.
- I would give this 3 word history = “New chest pain”.
I would then ask 2 Questions:
- Question #1: Should you activate the cath lab?
- Question #2: How LONG did it take to determine your answer to Question #1?
If your colleague (be he or she physician of any specialty, nurse involved in acute cardiac care, or paramedical personnel) answers within seconds with a resounding, “Yes, activate the cath lab” — You can take comfort in knowing that your colleague appreciates the shortcomings of the outdated STEMI paradigm — and that your colleague has clearly learned to recognize acute coronary occlusion in optimal time-efficient fashion regardless of whether or not frank ST elevation is present on the initial ECG.
= = =
Today’s initial ECG …
Why should we be able to recognize within seconds that today’s patient, who presents to the ED with a 2-hour history of acute CP (Chest Pain) and the initial ECG that is shown above in Dr. Smith’s discussion needs prompt cath?
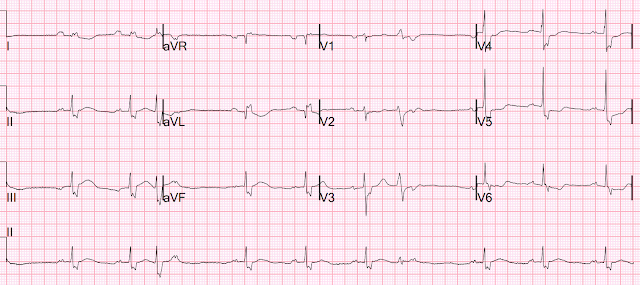
- My answer to this question is readily apparent in Figure-1 — in which I have labeled KEY findings in the initial ECG.
= = =
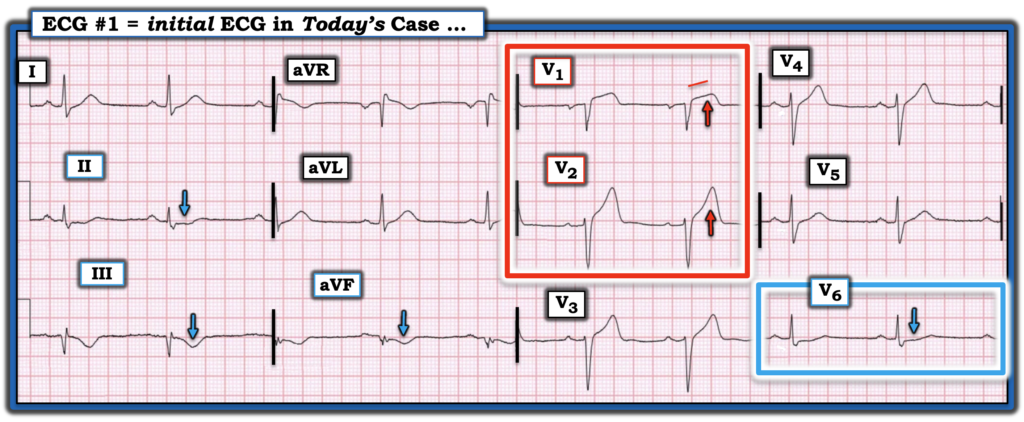
Figure-1: I’ve labeled KEY findings in today’s initial ECG.
= = =
Acute OMI with Precordial “Swirl“
Given this patient’s age (ie, “60-something” ) and the history of new-onset CP — this man immediately falls within the category of higher-risk for having an acute cardiac event. As a result — our “threshold” for recognizing any suspicious ECG findings as abnormal is heightened.
- My “eye” was instantly captured by the 2 leads within the RED rectangle in Figure-1 because — i) Normally there is little if any ST elevation in lead V1 — which means that the straightening of the ST segment takeoff and disproportionate amount of ST elevation (considering the very small size of the S wave in this lead) is clearly abnormal; — and, ii) The size and overly wide base of the T wave in lead V2 is clearly disproportionate considering modest depth of the S wave in this lead.
- As per Dr. Smith — the diagnosis of Precordial “Swirl” is secured by the finding of ST segment flattening and depression in lead V6 (within the BLUE rectangle in Figure-1).
- Confirmation of acuity is forthcoming from reciprocal changes in the inferior leads (disproportionate “bulkiness” of the inverted T waves in leads III and aVF).
= = =
Conclusion: With experience — Total Time to recognize the above ECG findings in this patient with a high-risk history should be seconds. There is no need to wait for Troponin values — and really no need to delay for a repeat ECG since regardless of what may transpire during the ensuing minutes or hours of this case — this patient has an acute OMI until proven otherwise in the cath lab.
- In addition to the 20 Cases of “Swirl or Look-Alikes” in the October 15, 2022 post in Dr. Smith’s ECG Blog — I synthesize the KEY points for rapid recognition of Precordial Swirl in My Comment at the bottom of the page in that October 15, 2022 post.
= = =
= = =