By Pendell Meyers
A man in his 60s presented with acute pain of the shoulders, neck, throat, and jaw following rigorous physical activity without trauma. He adamantly denied any “chest” pain or discomfort. His triage vital signs were within normal limits.
Smith: 33% of acute MI have no chest pain. Unexplained shoulder, neck, or throat pain is angina/MI highly suspicious for acute MI.
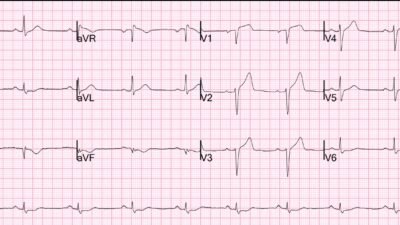
Here is his triage ECG with active pain at 1700:
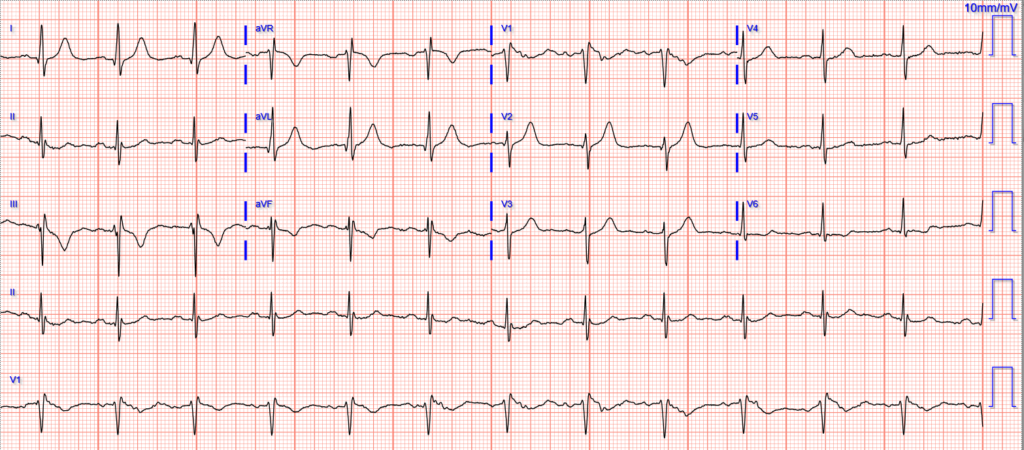
There is sinus rhythm with a reasonably normal QRS complex. There is no diagnostic ST elevation, but there is a hint of ST depression in V3 and V6. There are abnormally large T waves in I, aVL, and V2, with likely abnormal T wave inversion in III and aVF. If these findings are due to OMI, then the question is whether they represent inferior reperfusion, or high lateral active coronary occlusion. Of course, we know that the patient has active chest pain, so that greatly favors high lateral active OMI rather than reperfusion (which is usually associated with improved or absent symptoms).
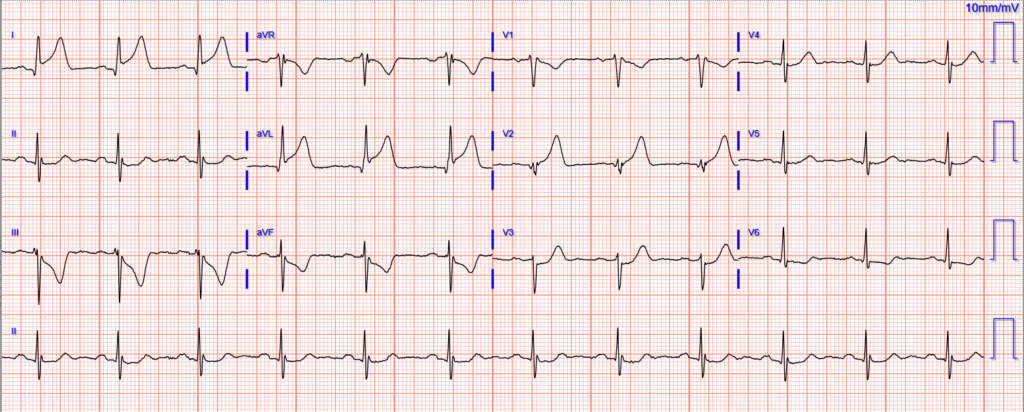
Here is his baseline ECG available from months ago (without any ACS event at that time):
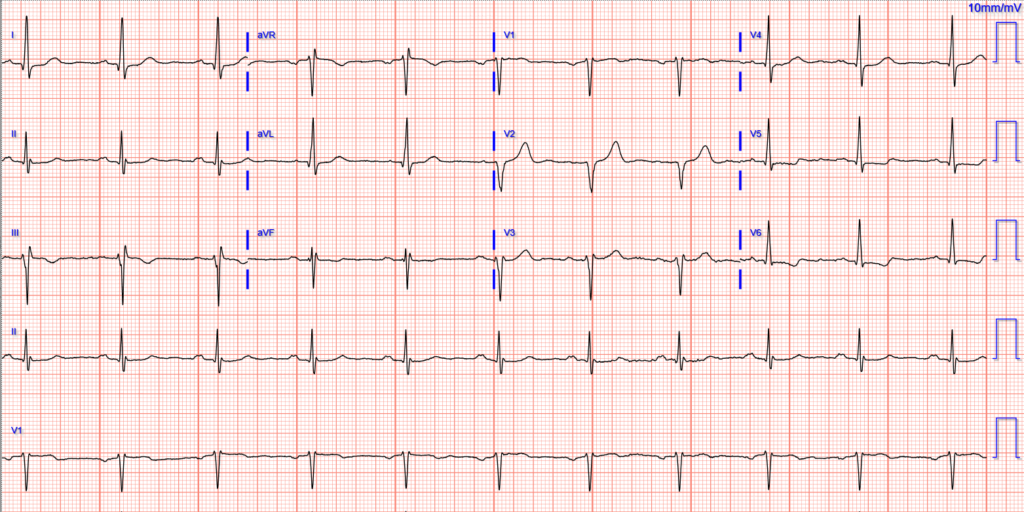
The physician read the ECG as “No STEMI or OMI. Does have T wave inversions in lead III and aVF which have not been seen previously.”
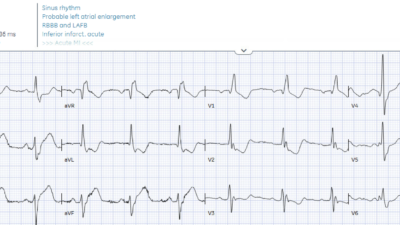
Here is Queen of Hearts interpretation on the initial ED ECG:
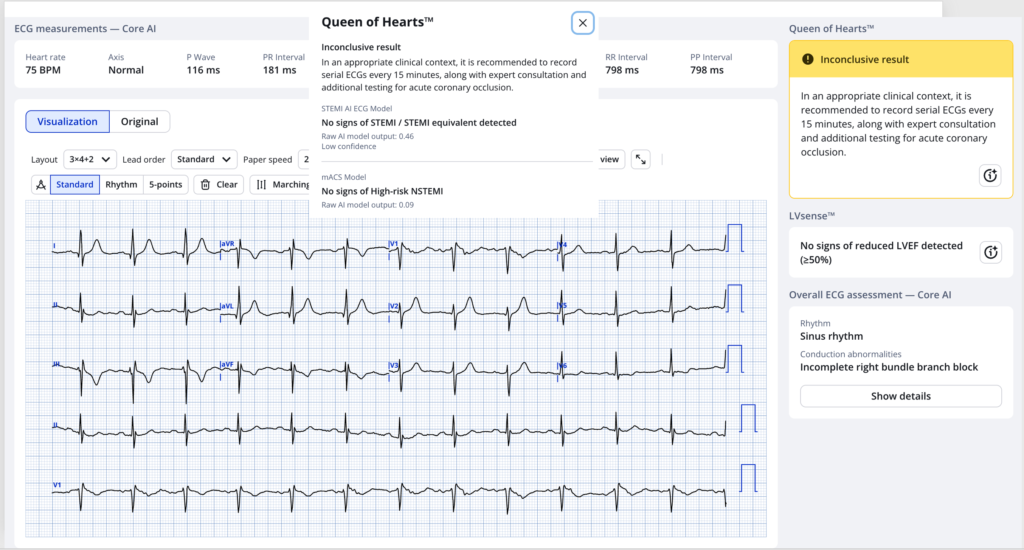
As you can see, the AI score is 0.46. Above 0.50 is diagnostic of OMI. So this is nearly diagnostic and so we label it “Indeterminate zone for OMI.” This is a very high risk situation when the clinical situation is concerning for ACS. This result is right on the border of showing a positive/diagnostic result.
HATW Score: 0.85 (>=0.70 is positive)
Leads I and aVL (and V2) have T waves that meet our formal HATW formula, specific for OMI.
Here is Queen of Hearts on the baseline ECG:
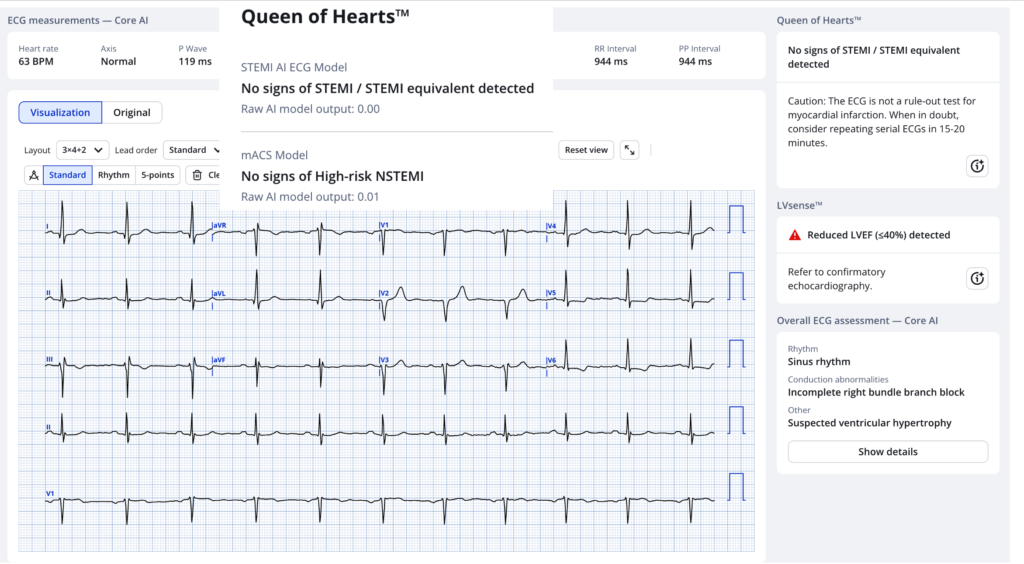
0.00 out of 1.00. As low as it gets for QOH.
A change from 0.00 to 0.44 is a huge change, and very concerning. QOH does not yet automatically incorporate serial ECG or baseline vs. acute ECG analysis. The clinician must still do that for now until future versions.
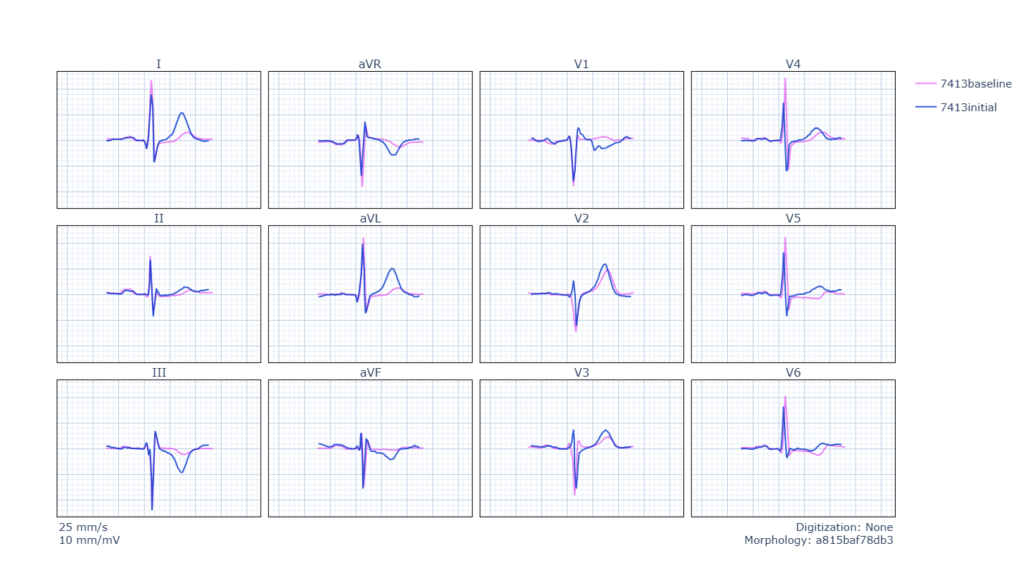
Here they are superimposed on each other (pink is baseline, blue is ED triage)
The ECG was deemed negative and he underwent musculoskeletal evaluation including CT cervical spine which was negative for acute fracture or traumatic injury. X-rays of both shoulders were done next and negative.
Troponin was ordered and resulted elevated at 102 ng/L.
At this time, the chart says:
“Patient was reevaluated, he continues to deny chest pain or shortness of breath at this time, just complains of continued anterior neck pain. However given the bilateral shoulder and jaw pain along with elevated troponin, will order repeat EKG, check delta troponin.”
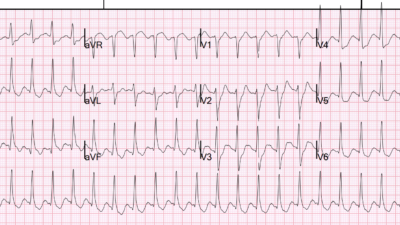
Repeat ECG 1849, 109 minutes after the first one (remember that the Queen recommended recording an ECG every 15 minutes!!):
Obviously STEMI+ OMI. South African Flag pattern.

“Unfortunately patient’s second EKG shows evidence of development of a STEMI at this time in the lateral leads, lead I and aVL. Reciprocal changes with T wave inversions in 3 and aVF. Code STEMI was initiated at this time…”
Angiogram at 2017:
D1 99% culprit lesion, PCI performed
Echocardiogram:
Wall motion abnormalities: hypokinesis of mid to apical anterolateral myocardium, mid to apical inferolateral myocardium
Second troponin: 5,265 ng/L, (none further measured)
The patient survived the hospitalization.
Do you think his long term outcome (heart failure, longevity) would be improved if he had ~2 hours earlier treatment of his acute coronary occlusion causing STEMI on ECG???
I do.
Would you want your coronary occlusion treated 2 hours earlier than the STEMI ECG?
I think you would.
Learning Points:
We can find OMI earlier than STEMI criteria.
Serial ECGs are a good idea no matter how good you are at the ECG. Please don’t wait until positive troponin to order them.
“Subsequent ECG STEMI” like this case represents approximately 15% of all STEMIs (data forthcoming)
Even if you only care about STEMIs (not NSTEMI-OMIs), please think about how you can find these cases faster with better ECG interpretation.
Stay tuned for our multicenter 1000+ patient study on this topic coming soon.
= = =
==================================
MY Comment, by KEN GRAUER, MD (6/12/2026):
Today’s case by Dr. Meyers highlights how the need for prompt cath can (and should) be recognized not only before a STEMI develops — but at times, even before acute OMI is diagnosed.
- Providers were led astray in today’s case by the lack of CP (Chest Pain). That said — it is well established that not all patients with acute MI develop CP. Today’s previously healthy 60-year old man presented with acute new-onset symptoms (including shoulder, throat, neck and jaw pain) — that occurred following rigorous physical activity without trauma. As a result, rather than “reassurance” by the lack of CP — today’s history if anything, serves to increase concern, as it immediately places this patient in a higher-risk group for an acute cardiac event (especially given the continuation of “active pain” still present on arrival in the ED at the time the initial ECG in Figure-1 was recorded).
= = =
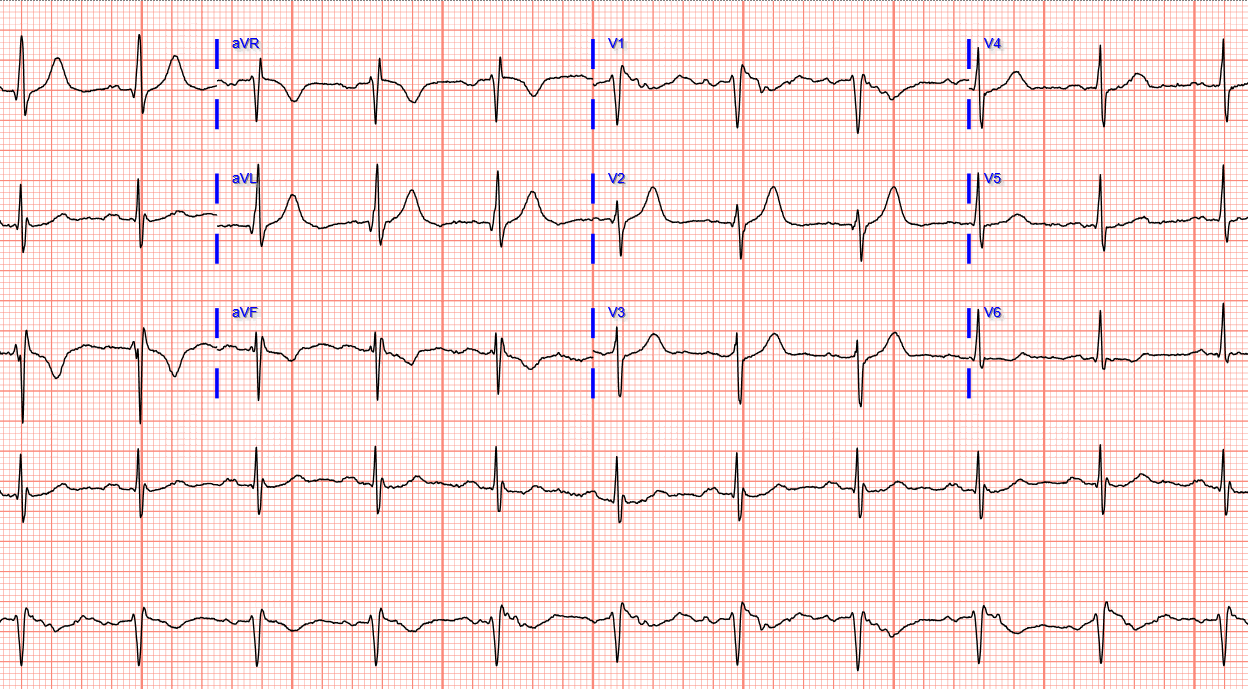
Today’s Initial ECG . . .
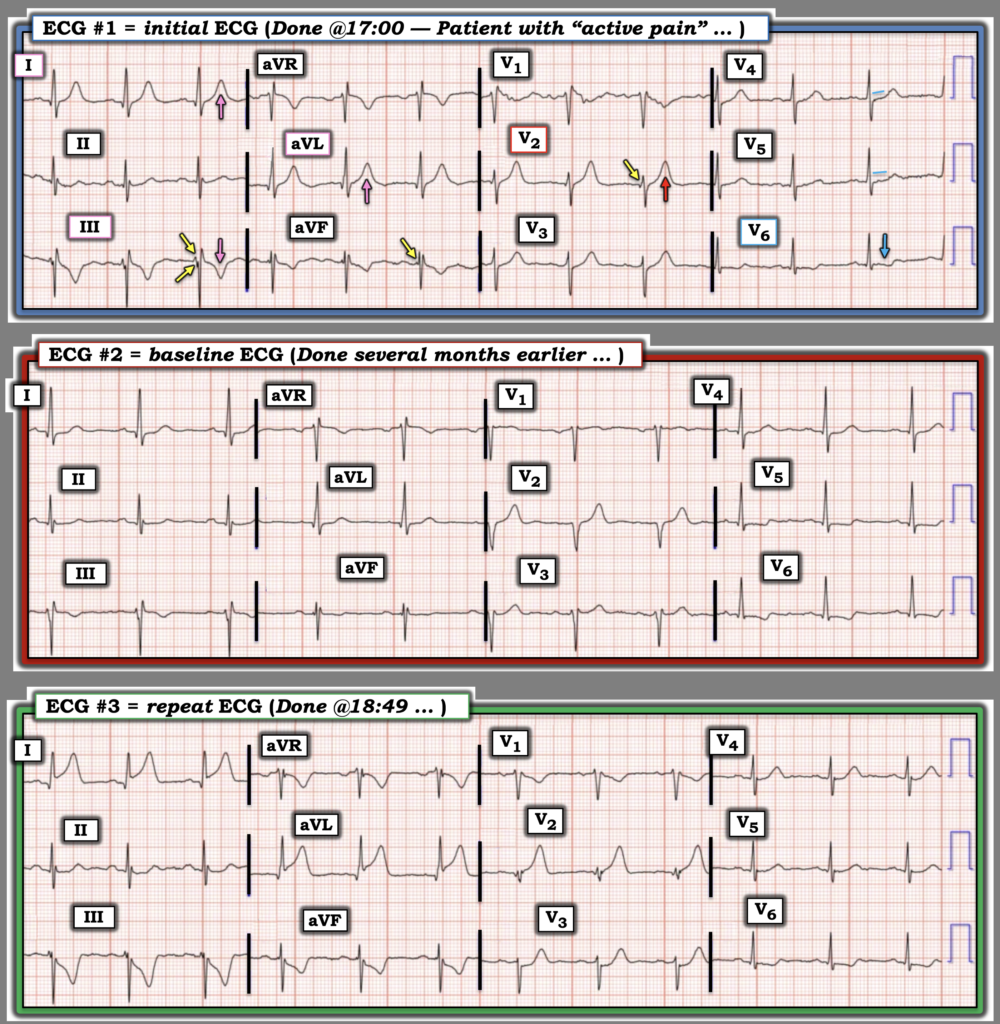
For clarity in Figure-1 — I’ve put today’s 3 ECGs together, labeling key findings in the initial ECG. Looking first at this initial tracing:
- The rhythm in ECG #1 is sinus at ~75/minute. The PR interval is normal — the QRS is narrow — and the QTc is not prolonged. There is no chamber enlargement.
- An rSr’ is present in lead V1 (? Incomplete RBBB — given small, narrow terminal s waves in leads I,V6) — with artifact in the lead V1 baseline precluding determination of whether Brugada phenocopy might have recently been present (See My Comment in the January 13, 2025 post regarding Brugada Phenocopy).
- Of note is the subtle fragmentation of the initial portion of the QRS in leads III and aVF (YELLOW arrows in these leads) — raising the question of whether this patient may have had inferior infarction at some point in time.
- There is also suggestion of loss of r wave from lead V1-to-lead V2 — potentially representing a very small infarction q wave in lead V2 (YELLOW arrow in lead V2).
The above said — What caught my “eye” was the following:
- The T wave in lead V2 looks disproportionately increased in size compared to the modest S wave depth in this lead (RED arrow in V2).
- Almost as marked is the disproportionate size of the upright T waves in leads I and aVL, and the negative T wave in lead III, especially given the absence of T wave inversion in lead II (PINK arrows in leads I,III,aVL). While T wave inversion may at times be seen when the QRS is predominantly negative in lead III — I thought the T wave inversion in lead III of ECG #1 to be inappropriately deep.
- While J-point ST elevation is not seen in leads I,aVL or V2 — the unexpected T wave prominence in leads I,III,aVL and V2 made me wonder if these findings in ECG #1 might represent an early South African Flag Pattern (See My Comment in the January 18, 2025 post— for review and illustration of the S. African Flag sign).
- In support of potential LAD and/or 1st or 2nd Diagonal OMI in this 60-year old man with ongoing pain from new-onset symptoms — is the ST segment flattening with slight depression that is clearly present in lead V6 (and to a lesser extent in lead V5).
- Finally — there is ST elevation in lead aVR — which in association with the ST-T wave flattening/slight depression in the lateral chest leads suggests a component of DSI (Diffuse Subendocardial Ischemia) — potentially a result of multivessel disease.
- And I wondered what a previous ECG on this patient might show?
BOTTOM Line: While non-diagnostic — I thought ECG #1 to be highly suspicious of an ongoing acute event that most probably will merit prompt cardiac cath:
- As per the QOH interpretation — serial ECGs (every 10-20 minutes) are indicated — along with serial Troponins and finding a prior ECG to facilitate determining what is new vs old.
- Given the worrisome history in today’s case, with ongoing pain — an emphasis on timely confirmation of the need for prompt cath is needed (ie, Any sign of Troponin elevation or “dynamic” ST-T wave change on serial ECGs or obvious new ST-T wave findings compared to a prior ECG should be enough to confirm the need for prompt cath).
= = =
Figure-1: Comparison between the 3 ECGs in today’s case.
= = =
A previous ECG is found …
Side-by-side comparison in Figure-1 between today’s initial ECG and the baseline ECG that was found from several months earlier — facilitates recognition of significant acute changes in ECG #1:
- The ST-T changes highlighted by the PINK arrows in the initial ECG are all new compared to the baseline tracing. In addition, I thought the T wave prominence in lead V2 of ECG #1 was also increased. Given new-onset symptoms — I thought this supported my suspicion of a South African Flag pattern — such that the need for prompt cath was confirmed as soon as this prior baseline tracing was found.
- Other subtle findings suggested by comparison between ECG #1 and ECG #2 include: i) Similar subtle fragmentation at the onset of the QRS in leads III and aVF in the baseline tracing — suggesting the possibility of previous inferior infarction; — ii) No sign of ST elevation in lead V1 on the baseline tracing — supporting the possibility of a resolving Brugada phenocopy from ischemia on the initial ECG; — and, iii) ST-T wave flattening/depression in leads V4,V5,V6 was more prominent on the baseline tracing from several months earlier — suggesting significant coronary disease was probably already present at that time.
= = =
The repeat ECG (done almost 2 hours after ECG #1):
As per Dr. Meyers — the repeat ECG (that was only done 109 minutes after the initial ECG) — showed an obvious STEMI with a now fully developed South African Flag Pattern (consistent with the 1st Diagonal OMI found on cath).
- As is often the case — it’s insightful after you know cardiac cath results to go back to the initial tracing to better appreciate how initial ECG findings provided subtle clues of what was to come. I always learn from seeing how the initial ECG evolved.
- As per Dr. Meyers — We need to learn from this case how the need for prompt cath could have (should have) been confirmed several hours earlier than the time that it took.
= = =
= = =
= = =