One of our residents texted me this ECG and was worried about Wellens’ waves.
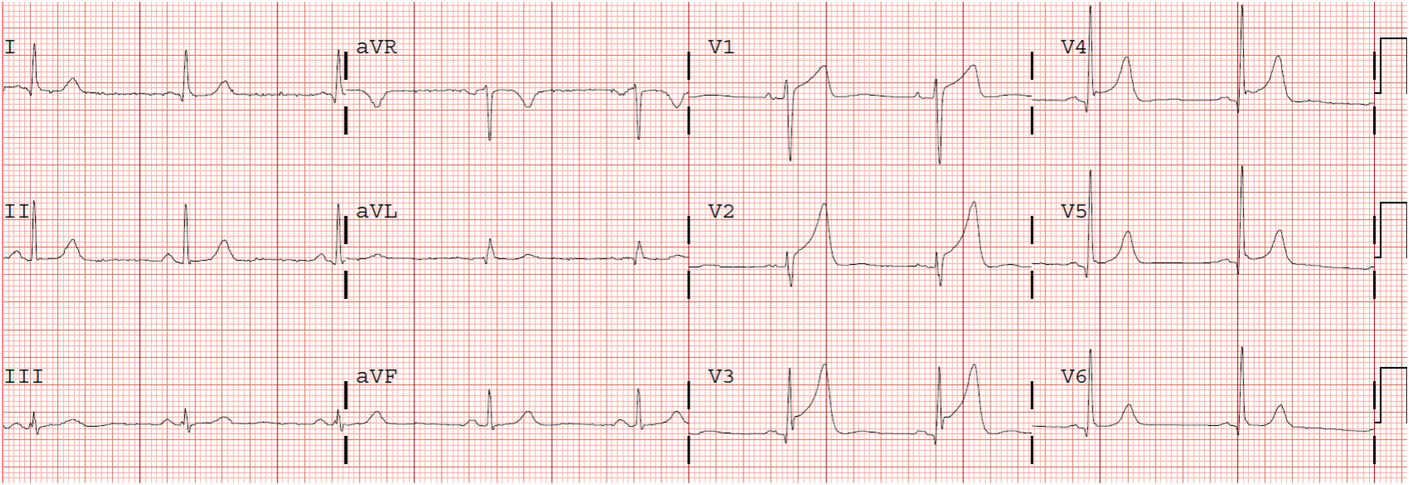
A middle-aged male presented with vomiting. Here was the initial ED ECG:
 |
| What do you think? |
Here is my response:
Wellen’s waves are always Up-Down T-waves, not Down-Up T-waves as here. Down-Up T-waves in V2 and V3 have only two causes:
1) posterior MI with some reperfusion (reciprocal to Up-Down T-waves of the posterior wall, analogous to Wellens’ of the posterior wall as recorded from the anterior wall).
2) Hypokalemia (in which case the upright component is really a U-wave). In this case, V6 is pathognomonic: you can see a clear large U-wave following the T-wave. It must be hypokalemia. Notice also the very long QT, which is really a long QU-wave.
What is the Potassium?
The K was 2.0 mEq/L.
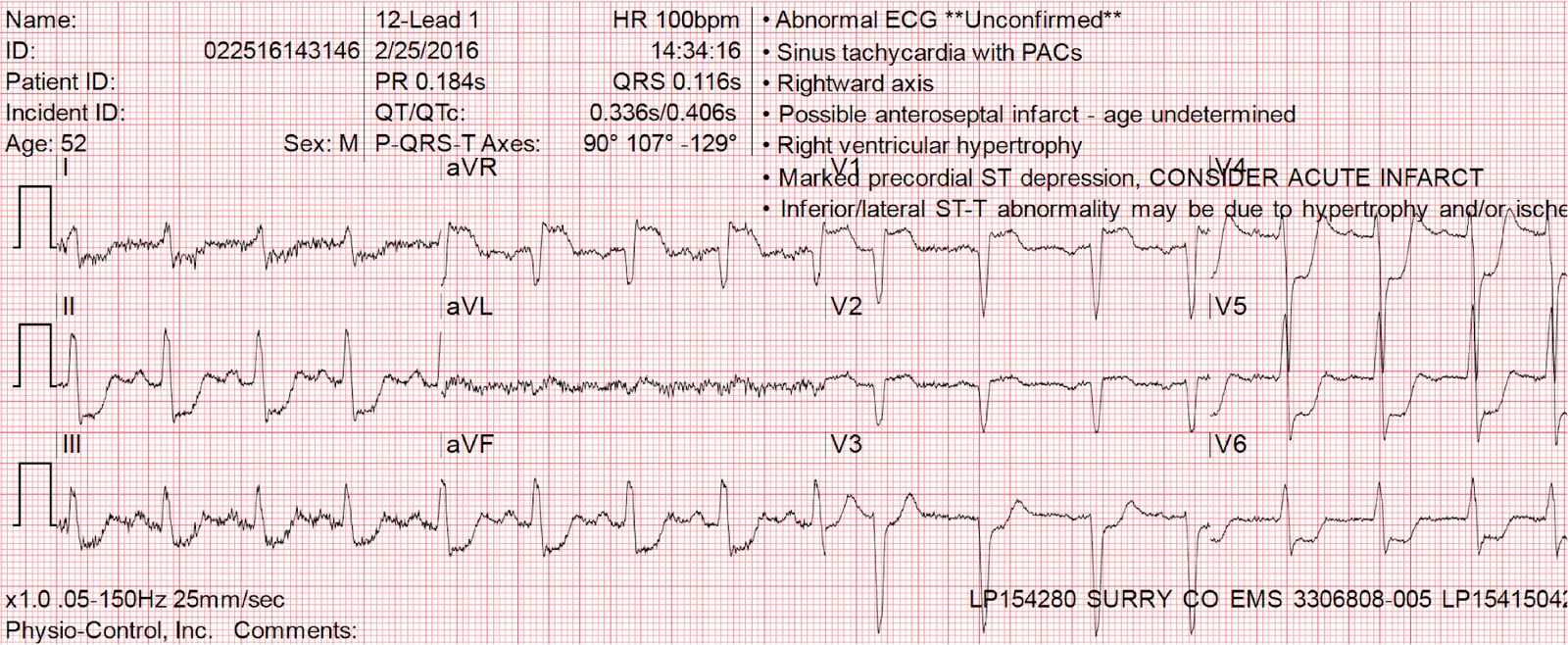
Here are classic Wellens Pattern A (biphasic) waves:
 |
| Notice they are biphasic Up-Down. |
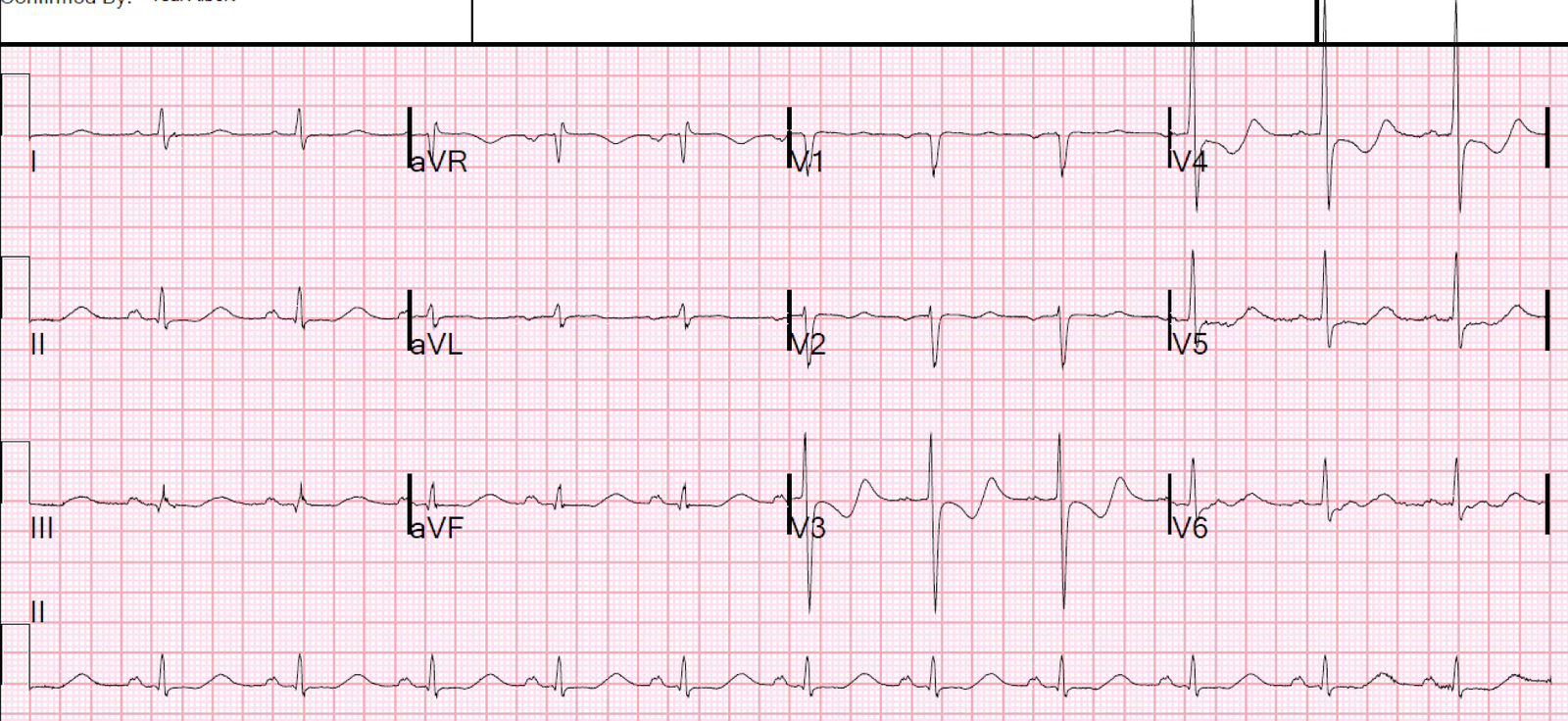
Clinical Course
The patient had all serial troponins below the level of detection. Potassium was repleted. Here is the ECG after normalization of K at 3.5 mEq/L:

Learning Points
1. Wellens’ waves (Pattern A) are biphasic Up-Down. (Pattern B is deep symmetric inversion)
2. Down-Up waves should make you think of reperfusing posterior MI or hypokalemia.
3. A very long QT (really a QU) should make you suspect hypokalemia.
4. Look for clear U-waves in other leads.
5. Finally, Wellens’ syndrome is a SYNDROME that requires 1) typical anginal chest pain 2) Resolution of the chest pain 3) ECG recorded after resolution.
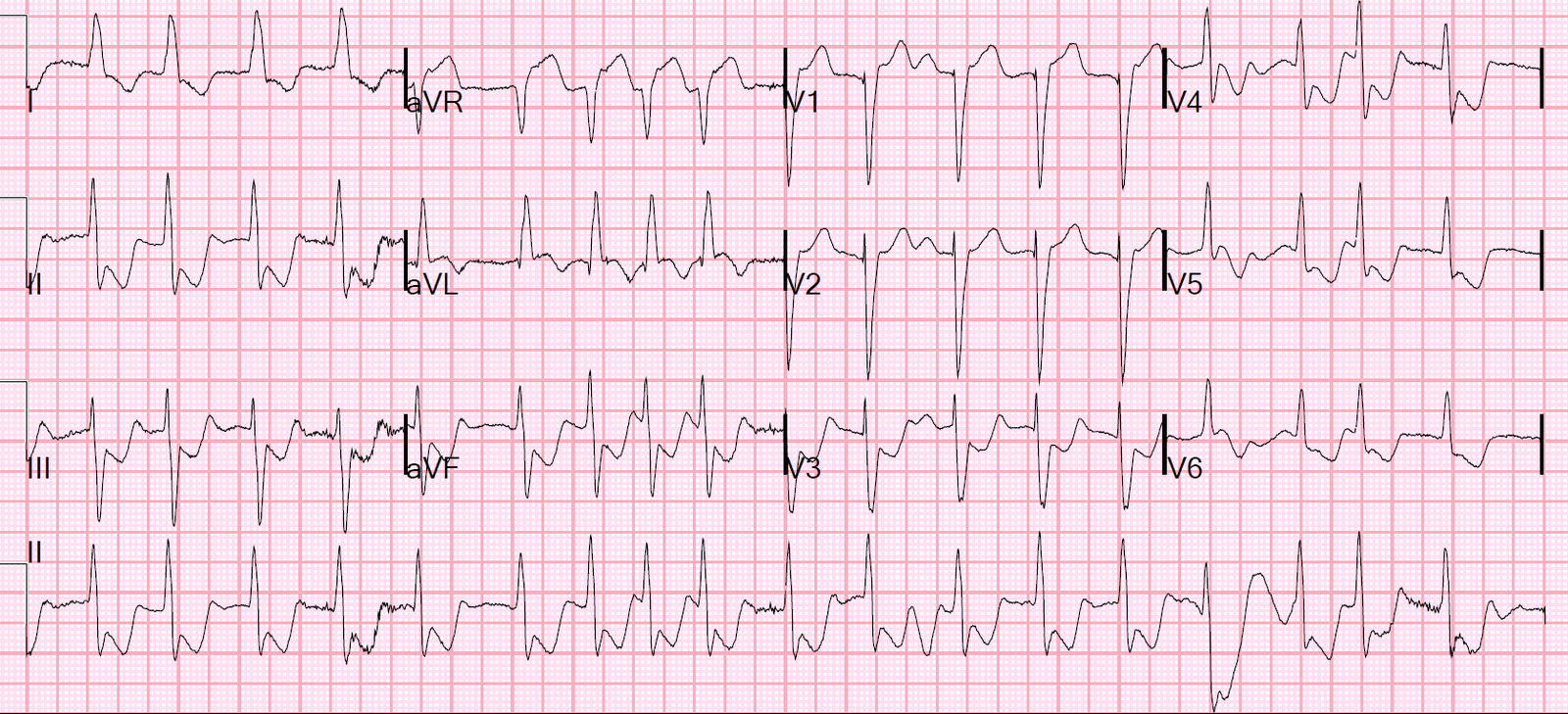
Here is an example of a Down-Up T-wave from Reperfusing Posterior MI.
It comes from this fascinating post:
Series of Prehospital ECGs Showing Reperfusion