This was provided by Mustafa Alwan, an internist from Jordan, on Facebook EKG Club
A 50-something female presented with atypical chest pain described as stabbing, with no radiation
PMHx : DM poorly controlled
VITAL signs stable
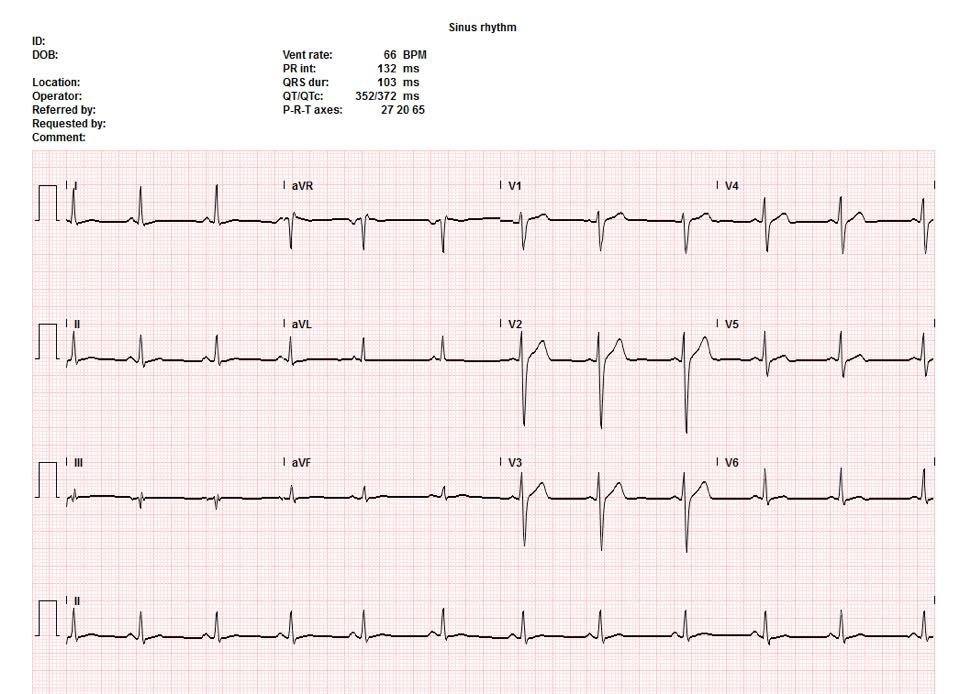
Here is the initial ECG with the question “should the cath lab be activated?”
 |
| This is suspicious for ischemia because of the T-wave inversion in aVL. However, this is very nonspecific and one would not activate the cath lab! |
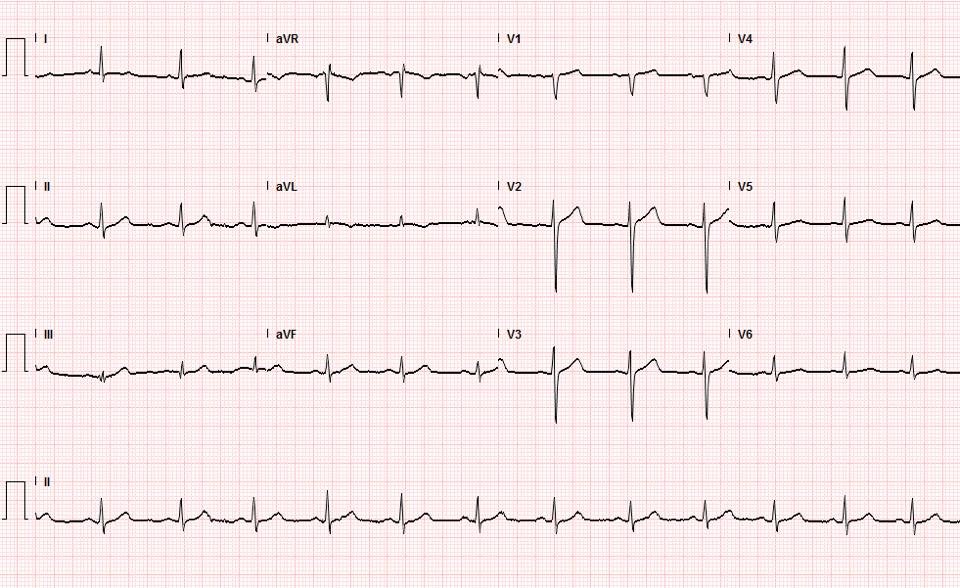
Another ECG was recorded 20 minutes later:
 |
| This has more obvious T-waves and T-wave inversion in aVL Here is my response: “This 2nd one is an extraordinarily subtle but real change!!” (i.e., this is diagnostic of MI). “These often resolve with nitro, so I would try that first. It depends on your resources: if activating at night tires out your team for the next day, you try to avoid if possible. But this pain and ECG may not resolve, in which case you must activate.” In other words, this is diagnostic of inferior MI, but not of STEMI, and may not need emergent cath lab activation. If the pain and ECG findings resolved with nitroglycerine, it will need at least maximal medical therapy and continuous 12-lead ST segment monitoring |
See these cases for the importance of ST segment monitoring:
https://drsmithsecgblog.com/search/label/ST%20Segment%20Monitoring
A third ECG was recorded at 45 minutes:
 |
| Now it is unequivocally diagnostic of inferior MI, even though it does not meet millimeter criteria for inferior STEMI. The cath lab must be activated. |
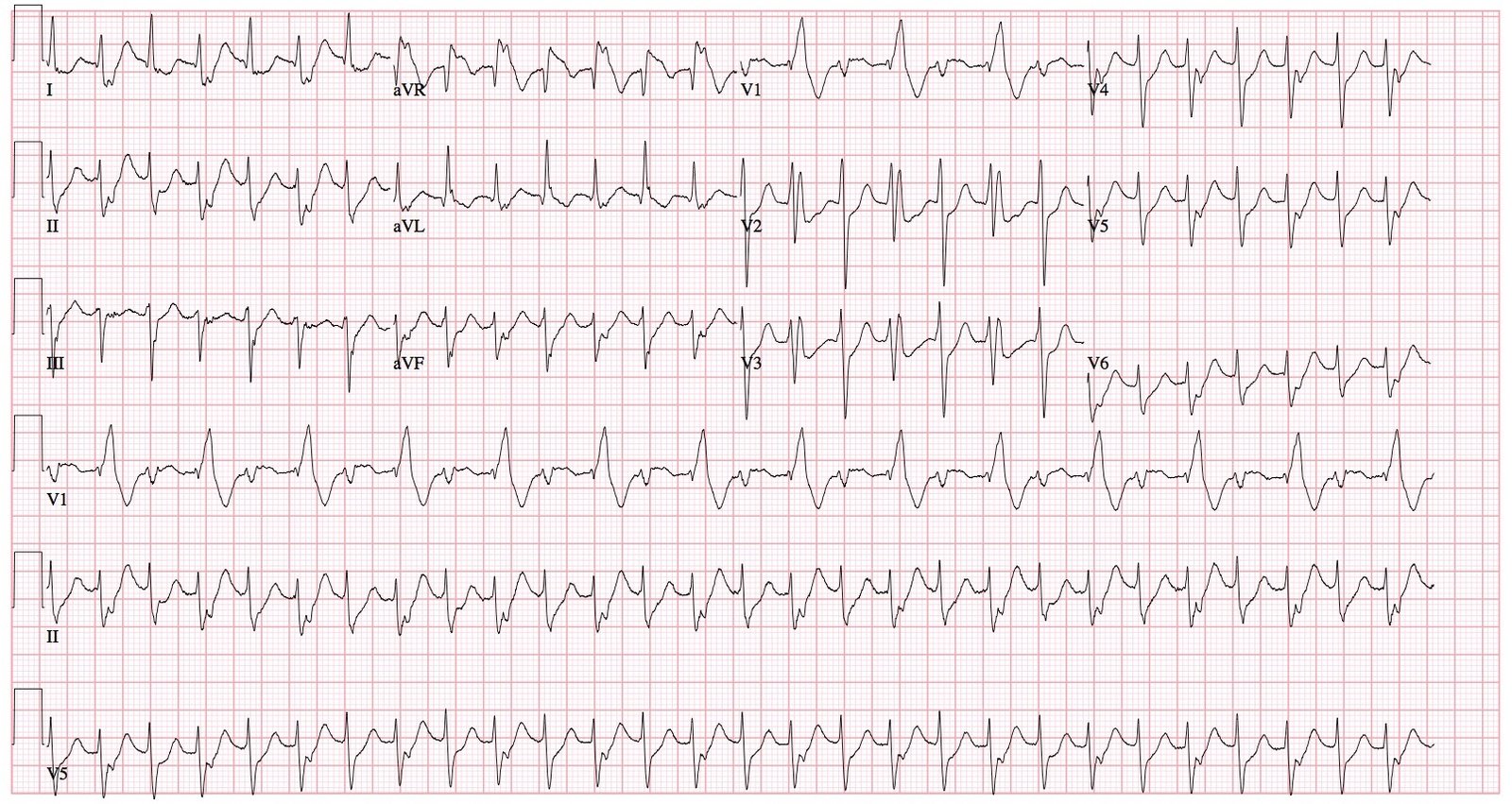
Here are all 3 ECGs, one after another, so you can see the changes:

The cath lab was not activated, but a 4th ECG was recorded at one hour:
 |
| Now it meets STEMI criteria. Cath lab was activated What else do you notice? |
There is also new ST elevation in V1. So this is a right ventricular MI also
Echo: Basal inferior wall hypokinetic, pseudonormal LV filling pattern
Initial Troponin T: less than 0.01 ng/mL initial
Troponin T after 2 hours: 0.49 ng/mL
Troponin T after 4 hours: 1.6 ng/mL (this is a large MI)
Cath showed a 100% proximal RCA occlusion.
Learning Points:
1. T-wave inversion in aVL may be the first sign of inferior MI
2. Pay attention to slightly enlarged T-waves
3. When you see these subtle, nonspecific abnormalities, make certain you get serial ECGs!
4. Any patient with ongoing potentially ischemic chest pain should get serial ECGs!