This piece was written by Brooks Walsh, who has some great contributions to this blog. There are, of course, some additions and edits by Steve Smith.
Cases
Two young adult males presented to the
ED with chest pain. An ECG was immediately performed in both cases. However, while one patient
received emergent PCI for an acute coronary occlusion (ACO), the other
only got a sandwich and ibuprofen.
Patient #1
 |
|
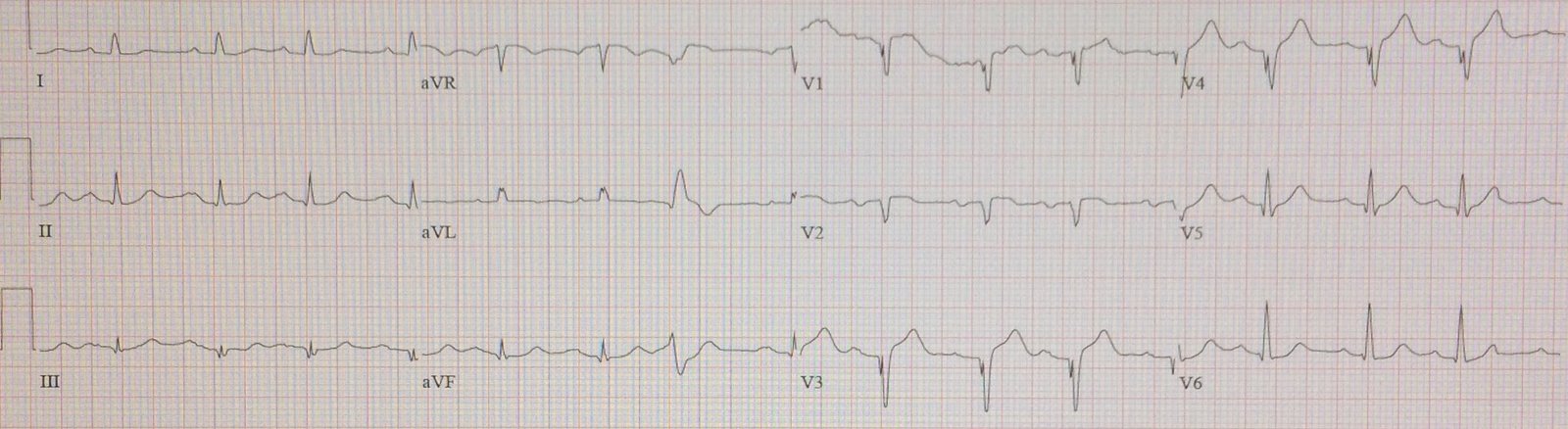
| There is ST segment elevation in multiple leads, most of which have an associated J-wave (slurring of the J-point); e.g. in V4-V6, I, II, and aVF. There is no reciprocal depression, the QTc is not significantly lengthened, and the ST segments in V2 – V4, although elevated, are concave upwards. All of these elements point to benign early repolarization. |
| If you used the LAD occlusion vs. Early Repol formula, using:
1) 3.0 mm for ST elevation, relative to PQ jct., at 60 ms after the J-point in lead V3 2) QTc = 405 ms 3) R-wave amplitude in V4 = 17 mm You get: 21.9, which effectively excludes LAD occlusion But you should not have used the formula for this case. Why not? (the answer is below)
See this post: 12 Example Cases of Use of 3- and 4-variable formulas to differentiate normal STE from subtle LAD occlusion
It has also been externally validated: A Tale of Two Formulas: Differentiation of Subtle Anterior MI from Benign ST Segment Elevation. Patient #2
|
| There is ST segment elevation in multiple leads, most of which have an associated J-wave (slurring of the J-point); e.g. in V4-V6, I, II, and aVF. There is no reciprocal depression, the QTc is not significantly lengthened, and the ST segments in V2 – V4, although elevated, are concave upwards. All of these elements point to benign early repolarization. |

Incidentally, the formula value here, using 4.0, 360 ms, and 30 mm R-wave, also excludes LAD occlusion. It equals 16.2
This is the
same interpretation as patient #1. What is the difference?
Take a
closer look at V3 in patient #2.
 |
| There is an S-wave which descends below the isoelectric line. This is a normal and expected finding. |
Even with
dramatic repolarization, lead V3 should manifest an S-wave. There are cases of early repolarization where the S wave is absent in V3, but
a J-wave is usually seen in those cases.
For
example, patient #2 had a second ECG recorded 10 hours after the initial
tracing:
 |
| Here, we don’t see an S in V3, but there is a clear “fish-hook” pattern to the J-point, consistent with BER. Serial troponins, were negative, and echo was normal, and serial ECGs (as shown above) did not evolve significantly. The diagnosis was pericarditis versus early repolarization. |
By
contrast, reexamine lead V3 in patient #1:
 |
| There is no S-wave in this lead, and neither is there a J-wave. This loss of the S-wave is called terminal QRS distortion, and multiple studies suggest that, with an anterior MI, this predicts a larger infarct, with higher mortality, and even a worse response to fibrinolytics or PCI. |
An old ECG was obtained for patient #1:
 |
| There is minor STE in V2-V4, and J-waves in leads II, aVF, and V4-V6. There is also an S-wave in V3! Thus, one should suspect that there is LAD occlusion obliterating the S-wave in V3. |
One hour
after the first ECG was recorded in patient #1, the troponin came back significantly
elevated, around 0.07 ng/ml (0.034 99th URL). A second ECG was
obtained:
 |
| There is no significant evolution from the first ECG, but cardiology was emergently consulted. Following a brief evaluation, the cath lab was activated. A 100% acute occlusion of the proximal LAD was found, and stented. |
Following
successful PCI, a third ECG was obtained. Note the re-appearance of the S-waves
in V3.
 |
| This immediate resolution of terminal QRS distortion bodes well for his clinical course, and indeed his follow-up echo was basically normal. |
Discussion
Dan Lee and I studied terminal QRS distortion and found that it was never present in any of 170 proven cases of normal variant ST Elevation (STE in Leads V2-V4).
Terminal QRS distortion is present in anterior myocardial infarction but absent in early repolarization.
The study from which the formula was derived only looked at ECG with “subtle” findings of LAD occlusion (as opposed to “obvious”). Of 355 LAD occlusions in both derivation and validation groups, 143 were “subtle” and were studied for the formula.
In the derivation group, the primary reason for excluding the ECG as “obvious” was terminal QRS distortion in 12 of 121 in the derivation group, and 28 of 234 cases in the validation group. Thus, in the first case, the formula should not be used because such cases with terminal QRS distortion were excluded.
The iPhone app for the formula asks you for exclusions. The sidebar LAD occlusion-BER calculator has red text above it outlining the exclusions.