This was sent to me by a medical student:
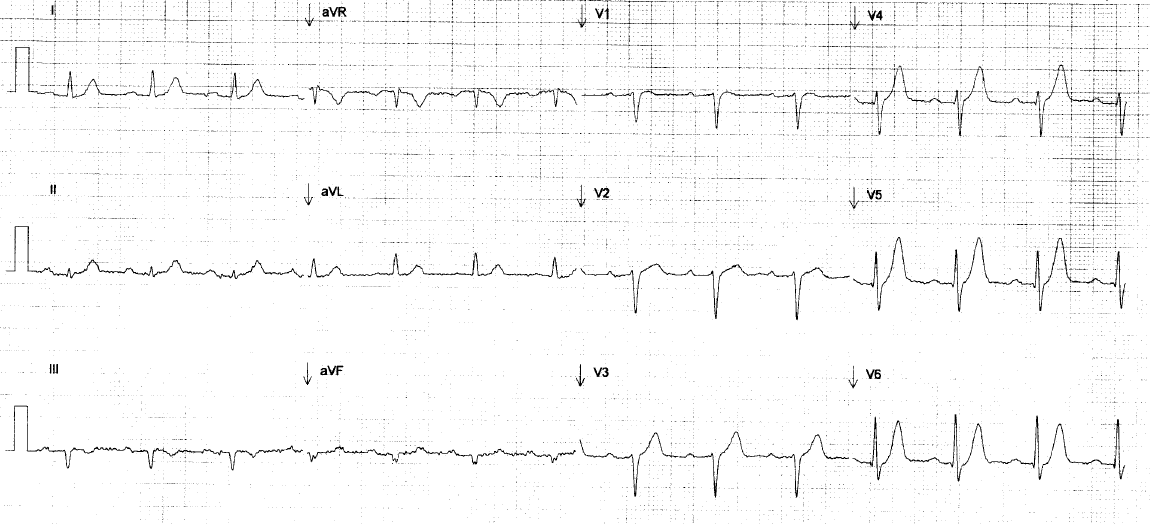
The patient is an elderly man with no significant past medical history who developed what he describes as chest tightness throughout his anterior precordium, 9/10 in severity, associated with nausea, vomiting, diaphoresis and shortness of breath, lasting for greater than 2 hours, that started while he was lifting firewood. His symptoms did not go away with rest. He presented to his primary care physician’s office. An EKG was recorded at 135 minutes after pain onset:
 |
| There is no old ECG for comparison. What do you think? |
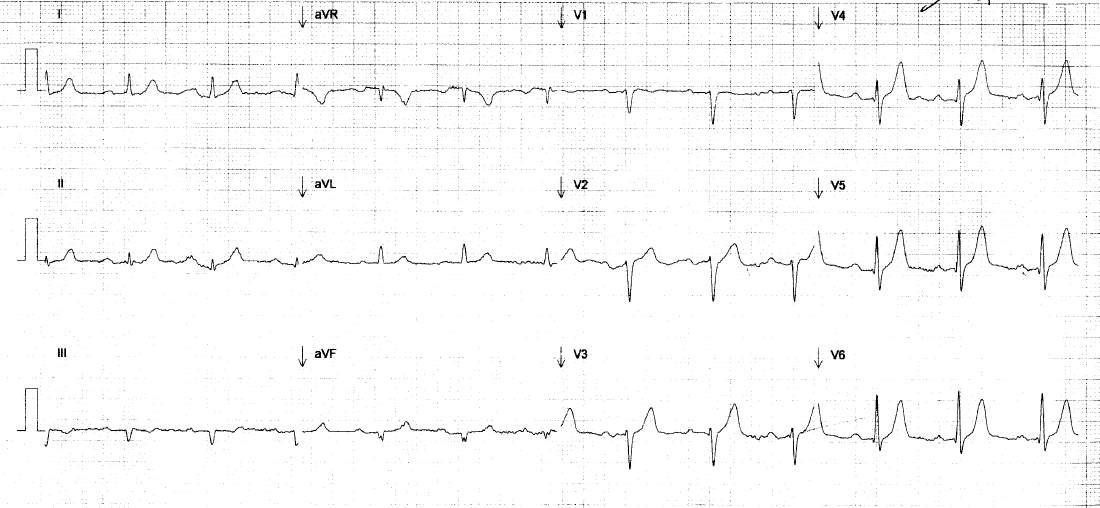
He was treated with sublingual nitroglycerin and aspirin, which improved his chest discomfort. He was transported by ambulance to the hospital. On initial evaluation in the emergency department he still had pain and had this ECG recorded at 150 minutes (2.5 hours) after pain onset:
 |
| What do you think? See below. |
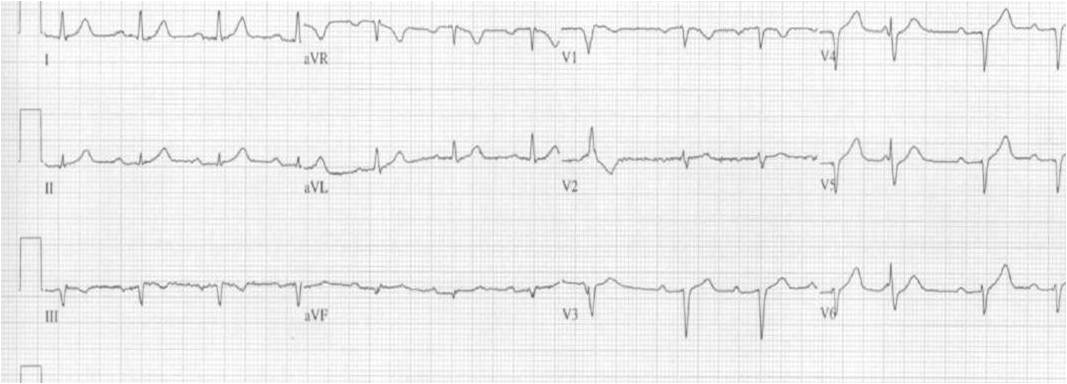
The med student asked what I thought, and I wrote: “hyperacute T-waves in V4-V6.” Here is the normal relationship between the T-waves and the QRS in V4-V6:
 |
| Knowing this is the normal proportion, what do you NOW think about the above 2 ECGs? |
It is clear that the T-waves in V4-V6 on the first two ECG are hyperacute. They are far too large for the QRS. In addition, if you look closely, you will see that there is more ST elevation on the second ECG. In fact, on the 1st ECG, V5 had zero ST elevation but has almost 2 mm on the 2nd ECG.
These findings, along with the pretest probability (a 77 year old with persistent substernal chest pressure and diaphoresis!!) mandate at least a stat formal echo, but preferably emergent coronary angiography
Initial cardiac markers were negative. The patient became chest pain-free.
He was admitted for a “rule out.”
A cardiologist evaluated his ECGs:
“In the emergency room an EKG was obtained which
showed Q-waves throughout the precordial leads and some reciprocal mild ST elevations but with a distinct J-point and less than 1 mm STE. I was asked to see the patient and review the ECGs and I felt this represented old anterior MI which had been completed at some point in the remote past.”
I do not fully understand this explanation.
He underwent more ECGs: 200 minutes (2 hours 40 min) after pain onset:
 |
| Complexes 8 and 12 are PVCs. R-waves in leads V4-V6 are much diminished and T-waves are not nearly as tall as they were. |
At 270 minutes (4.5 hours) after pain onset, the patient reported a slight increase in pain, and another ECG was recorded:
 |
| Now there is ST elevation in V4-V6, the T-waves are still large, and there is poor R-wave progression |
The cardiologist wrote this note:
“Pt reported a slight increase in pain. Repeat
EKG showed no clear ischemic changes. Old Q waves.”
At 10.75 hours after the pain onset, the pain was increasing. Troponin I returned at 7.42 ng/mL. This ECG was recorded:
 |
| Well developed infarction with QS-waves, diminishing T-waves and some terminal T-wave inversion |
Another ECG was recorded at 13 hours after pain onset:
 |
| Deepening T-wave Inversion |
At 15 hours after the first ECG, the patient was taken for angiogram and had a 100% distal LAD occlusion. It was opened and stented.
Here is the post cath ECG:
 |
| There is deepening T-wave inversion. |
Peak troponin I = 29 ng/mL. Formal echo shortly after the stent placement showed a dyskinetic anterior wall and an EF of 35-40%.
Learning Points
1. T-waves should be proportional to the QRS. If they are too large, you must suspect hyperacute T-waves and aggressively evaluate the patient with at least a high quality emergent echocardiogram
2. When the ECG is diagnostic, as here, do not wait for troponins to be positive before acting. Most coronary occlusion has initially negative biomarkers. Once the troponins are positive, much damage is done.