A 47 yo male presented to the Echo Lab one day after being seen in the ED for syncope. During the echocardiogram, the tech noted that the heart stopped. The monitor showed ventricular fibrillation. Before the patient could be defibrillated, he spontaneously reverted to an organzied rhythm:
 |
| Ventricular Fibrillation, then a period of asystole, then a slightly wide escape rhythm. One might question whether this is polymorphic VT, especially torsade. I have a very long strip and it is definitely ventricular fibrillation, also as read by an electrophysiologist. |
This happened several times before other personnel arrived with resuscitative equipment.
A 12-lead ECG was recorded:
 |
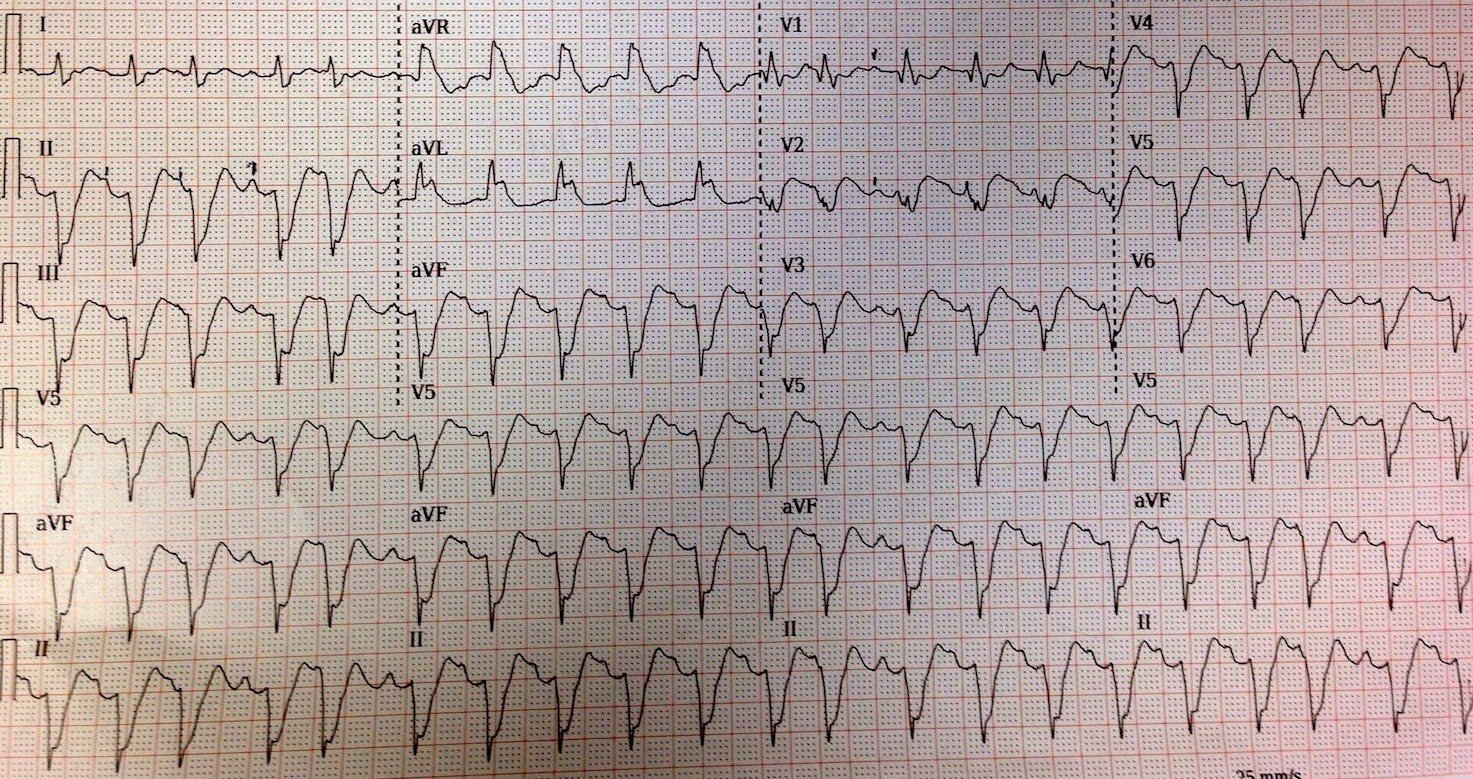
| There is no significant ST elevation, but there is ST depression in I, II, aVL and V4-V6. The QTc is 465 ms, just barely longer than normal and not enough to cause torsade. |
So the question comes up: what did he ECG look like at presentation to the ED the evening before? Here it is:
 |
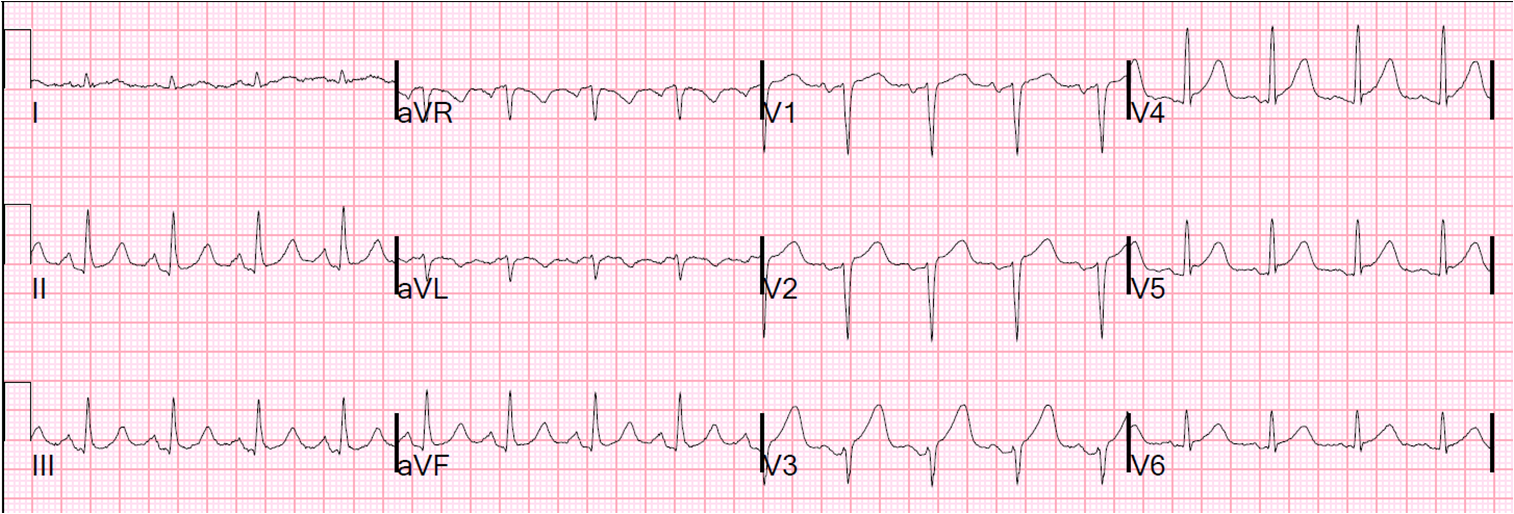
| Note how there is significicant ST elevation in V1 and V2 that is not there on the top (next day) ECG. Note also that the T-waves are very prominent on the ED ECG, unlike the next day ECG. The ST depression was present at that time as well. |
I applied the LAD Occlusion vs. Early Repol Formula to this ECG:
STE at 60 ms after the J point = 0.5 mm, computerized QTc = 460 ms, and R-wave amplitude in V4 = 7 mm; formula value = 25.45 which is greater than 23.4 and indicates that this is probably not normal variant ST elevation.
When the two are compared, it becomes clear that the ED ST elevation and T-wave are pathologic.
The patient was having anterior transient ST elevation ACS (technically not MI, as many have admonished me!!) at the time of the ED visit. Serial troponins were normal.
An angiogram showed “100%” mid-LAD but with very faint antegrade flow. He also had severe 3-vessel disease and underwent CABG 2 days later and did well. The artery was occluded or nearly occluded at the time of the ED ECG. This was the etiology of the ischemia and ventricular fibrillation.
Spontaneous reversion of V Fib:
Spontaneous reversion is a rare but documented cause of syncope. Here is one case report. I have spoken with two electrophysiologists who report seeing this in the electrophysiology lab. Frequently, what appears to be ventricular fibrillation is really polymorphic VT, as the two appear very similar morphologicially. More often, I am shows a strip of Ventricular fibrillation that along with an erroneous interpretation that it is “Torsade,” even though the patient was pulseless and required defibrillation. Torsade should only be diagnosed in the context of a significantly long QT on the baseline ECG. 465 ms is not long enough. Also, this morphology does not look like polymorphic VT (either Torsade or non-torsade PMVT).
Diagnosis:
1. ACS with 100% LAD occlusion
2. Syncope
3. Ventricular Fibrillation with Spontaneous