This was a middle aged female with a h/o CAD who presented to the ED by EMS sudden onset of central chest pressure 45 min prior to ED arrival with associated diaphoresis and SOB.
 |
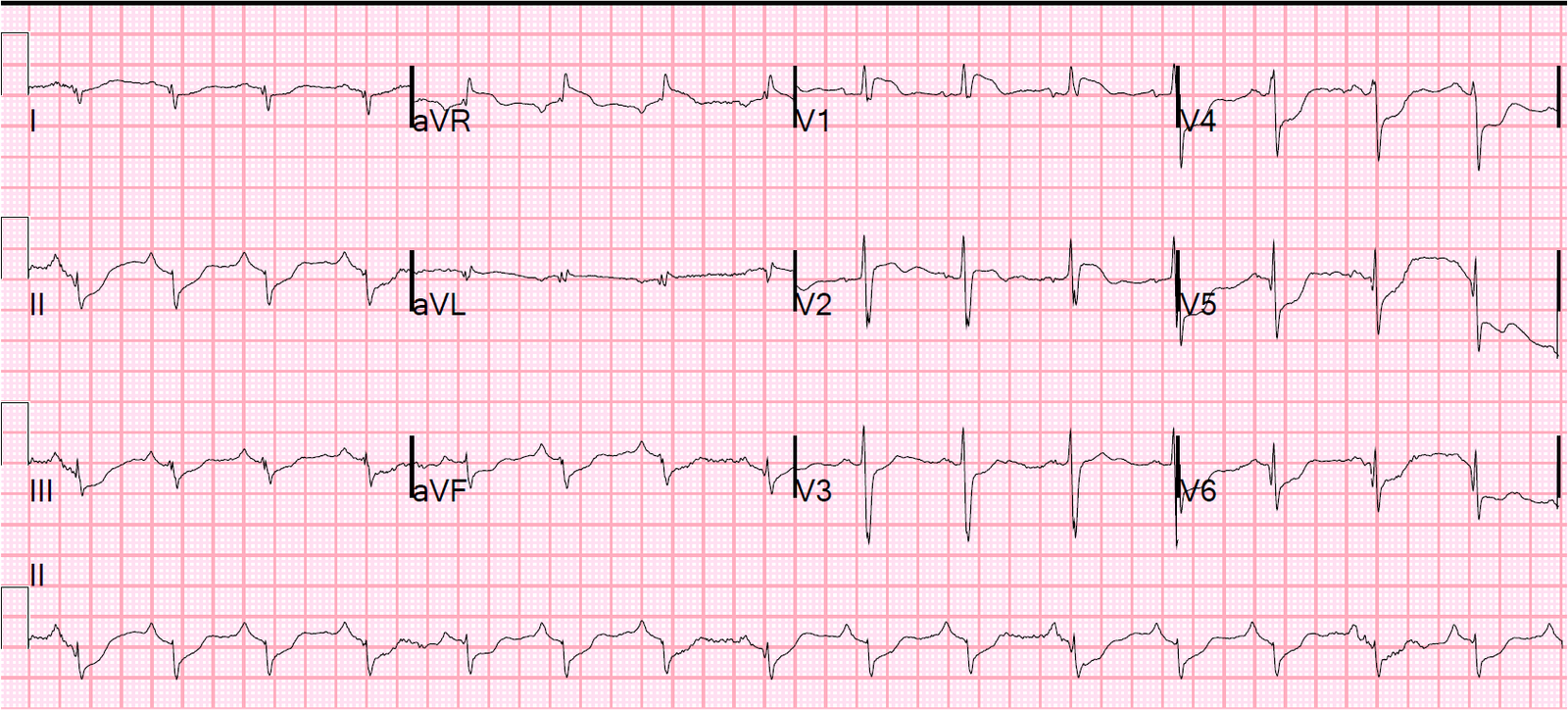
| There is LVH and there are ST-T abnormalities (large inferior T-waves and ST elevation, with reciprocal findings in aVL). There are also suspicious T-wave inversions in V2-V5; they look like Wellens’ waves in V4 and V5. Though the ST Elevation does not meet STEMI criteria, it is an obvious OMI. |
In LVH, just like in BBB, the ST segment (and T-waves) are often discordant to the majority of the QRS (ST elevated if QRS negative, as in inferior leads, or depressed if QRS mostly positive, as in I and aVL). Here is a previous post that demonstrates this.
In this case, the inferior ST elevation appears to be too much to attribute it to LVH alone.
The cath lab was activated but the interventionalist cancelled the activation.
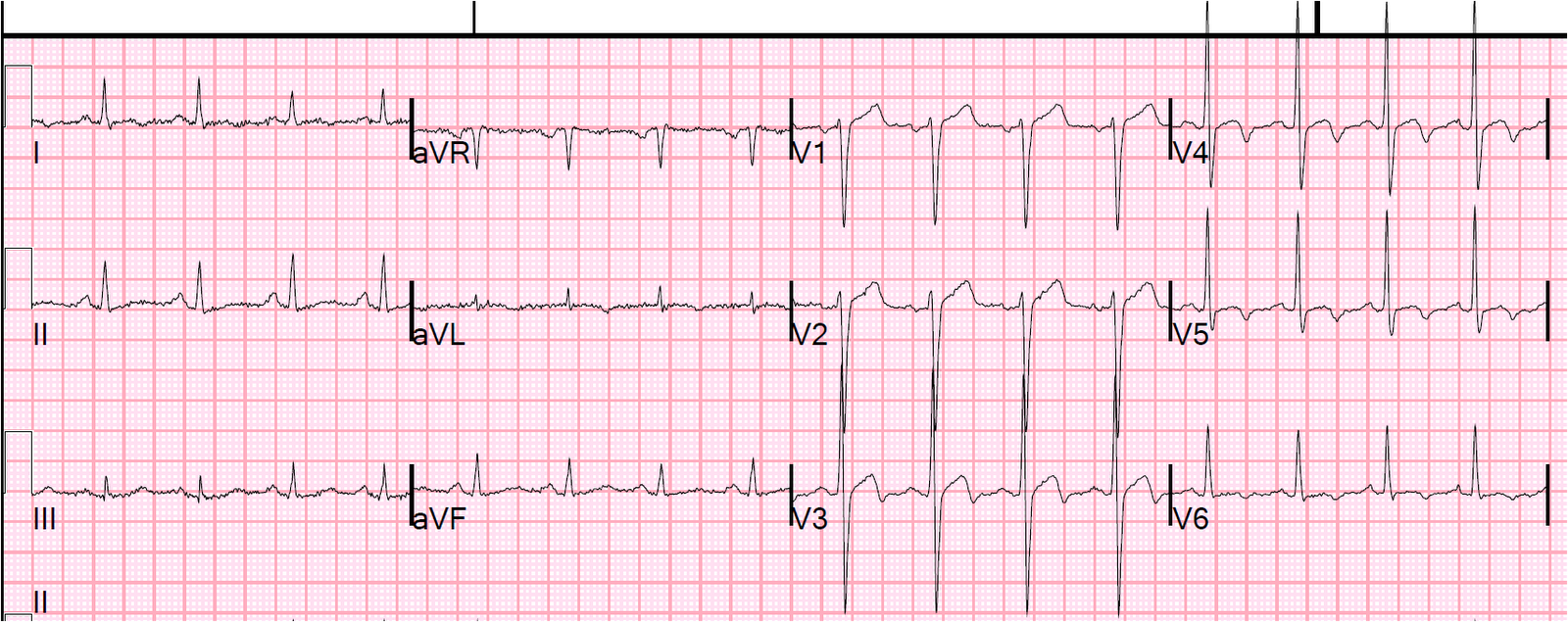
However, then a previous ECG was located:
 |
| Previous ECG has LVH in aVL, but no “secondary” ST-T abnormalities. This demonstrates that the precordial T-wave inversion is new as well. |
This confirms that the inferior ST elevation is new and thus due to acute OMI.
This case was written in 2012, before we changed the paradigm to OMI/NOMI and years before the Queen of Hearts was in use.
Now, in 2023, I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict:

The culprit was 100 % thrombotic occlusion of the mid RCA. The Peak troponin I was 47 ng/ml (equivalent to 47,000 ng/L) — a very large infarct. There was a regional wall motion abnormality in the inferior and posteriorior walls. The LAD was not involved.
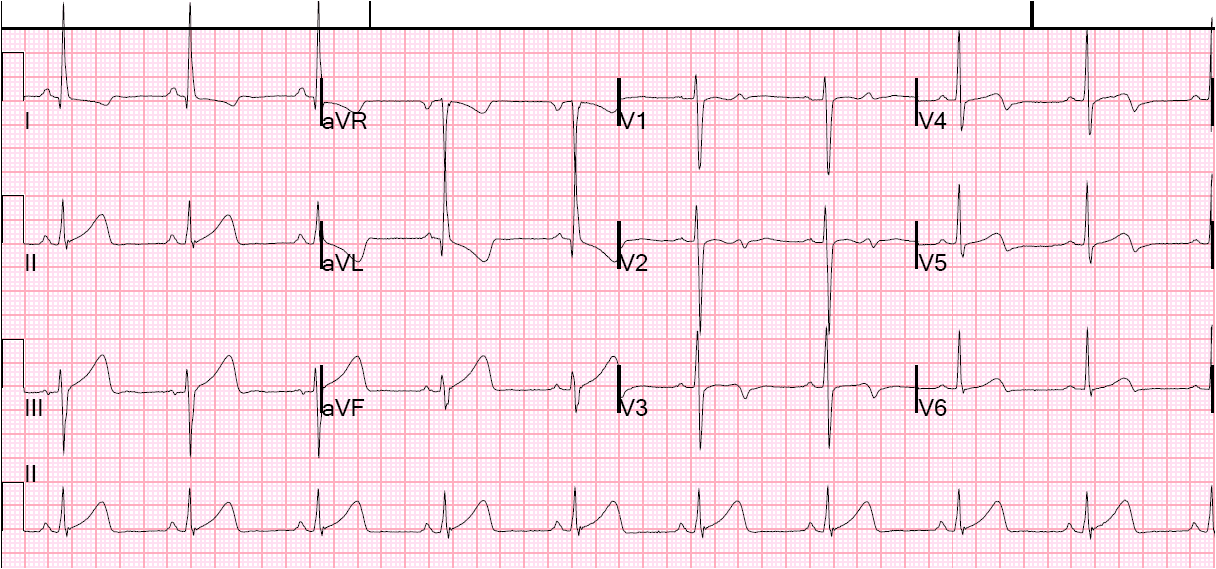
Here is the ECG after PCI:

This was called an NSTEMI by the cardiologists. Of what use is this nomenclature if a case such as this is called a NonSTEMI? There is occlusion of the infarct-related artery and ST elevation, but because it is not 1 mm at the J-point, it is arbitrarily called a NonSTEMI.
Had the patient not undergone immediate reperfusion therapy, much more myocardium would be lost.
That is why using any millimeter criteria for diagnosing STEMI is very insensitive (it is also nonspecific, as in LVH, BBB, early repol, etc.)