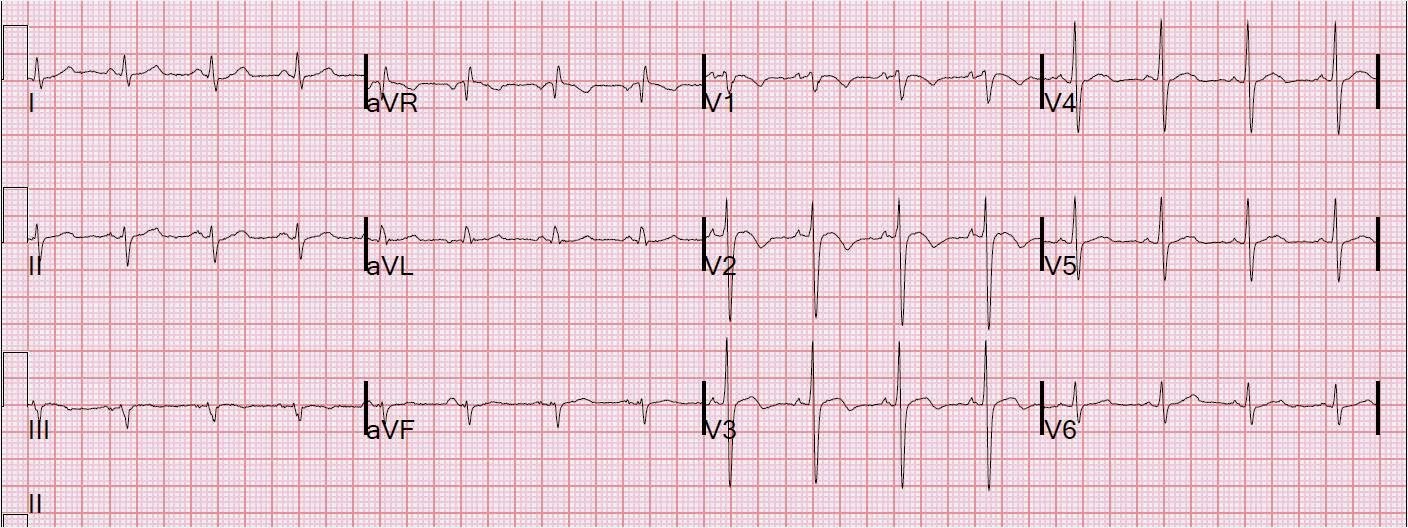
This 50 year old male presented with some atypical chest pain and a blood pressure of 220/150.
 |
| There is Left Bundle Branch Block with up to 6 mm of discordant ST elevation in V2 and V3. Limb leads have neither concordance nor discordance, and that is because the QRS is neutral: neither definitely positive nor negative. There are some biphasic T-waves in II and aVF, suggesting ischemia. The discordant ST elevation in precordial leads, though large, is proportional to a very high voltage S-wave (50 mm, or 5 mV). The ratio of the ST elevation as measured at the J-point = 6 divided by 50 = 0.12. The mean in my studies of LBBB without occlusion (either no MI or NSTEMI) was 0.10 +/- 0.1 (95% CI), so this is very close to a normal ratio. |
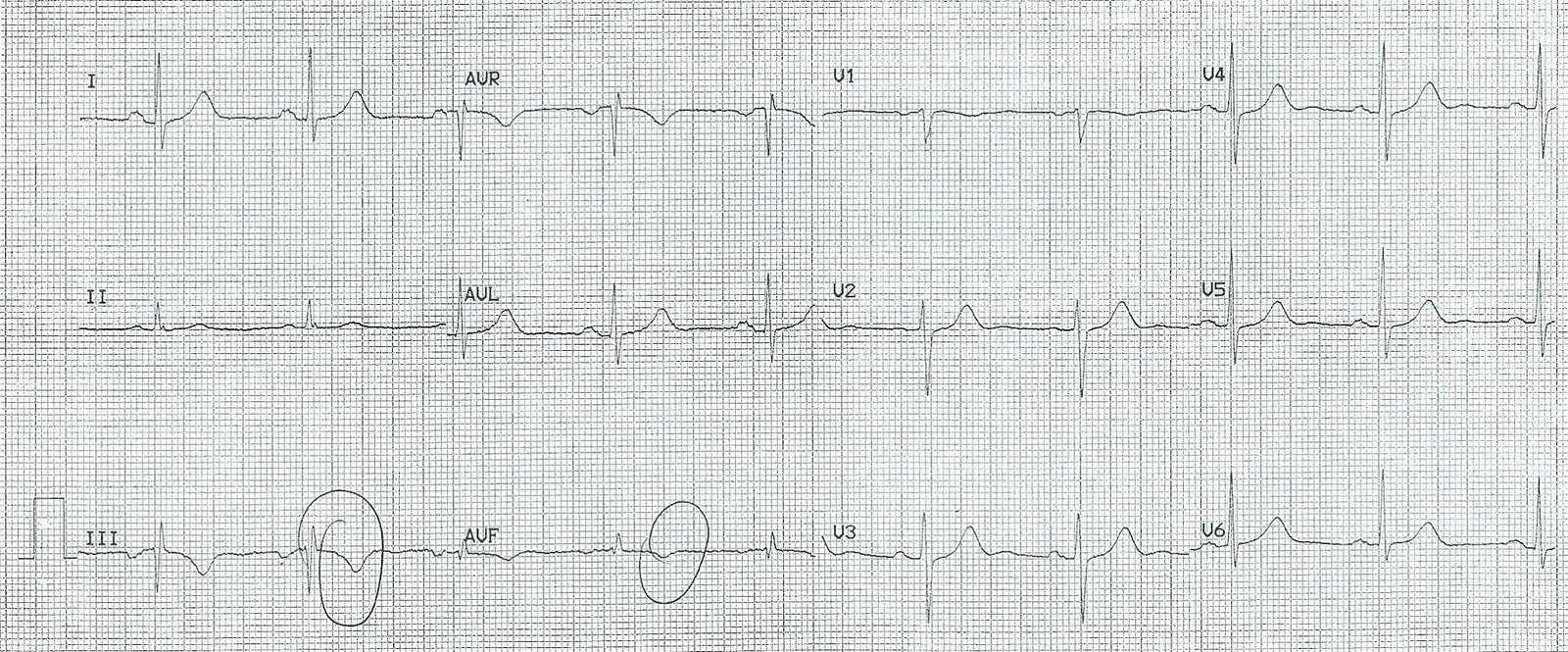
Here is the previous ECG:
 |
| This is a previous ECG from months ago, showing that the presentation ECG is indeed New LBBB. Here there is profound LVH with secondary ST/T abnormalities. |
This did not alarm me. In ED patients with symptoms of ischemia and New LBBB, only about 2-4% have acute coronary occlusion (need for immediate reperfusion therapy). Many more have MI as diagnosed by biomarkers. This is typical evolution of severe LVH to LBBB in a patient with severe HTN. There may well be MI as diagnosed by biomarkers, but it is not due to acute coronary occlusion, rather most likely to demand ischemia from severe hypertension (afterload, “type II” MI).
Troponin I had a rise and fall, but never went above the 99% reference value for the VITROS assay (in ng/ml): 0.017, 0.018, 0.029, 0.020. So this also represents a case that had some tiny amount of myocardial necrosis but is by current definition not an MI.