For more on computer misses, click here:
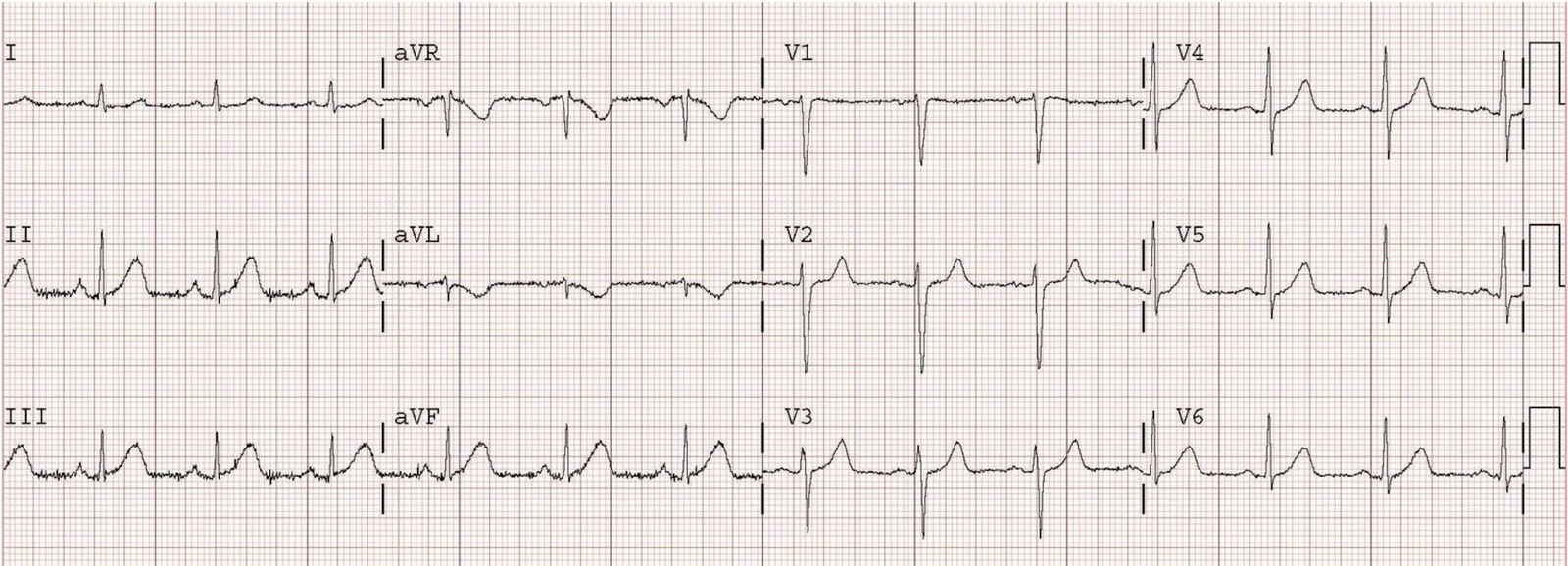
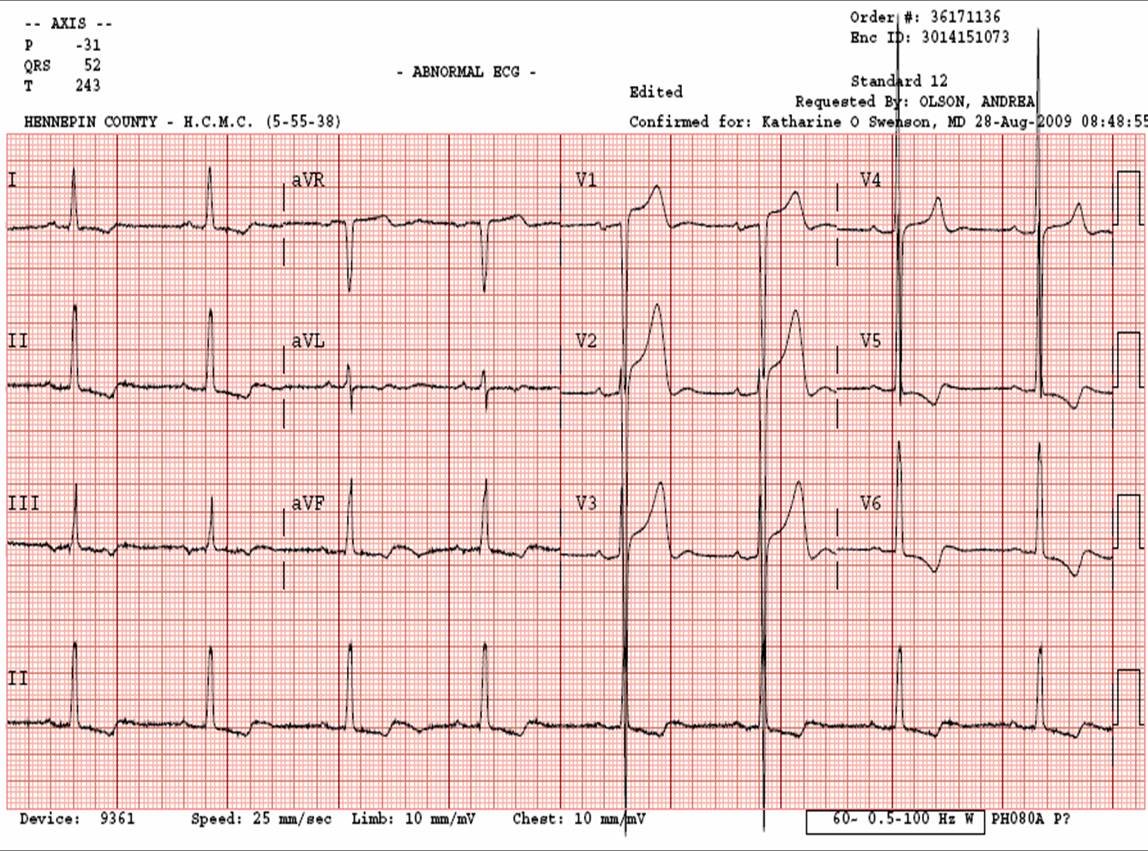
This is the prehospital ECG of a 37 year old male with chest pain. It is obviously an acute STEMI, and in this case involved a proximal wraparound LAD supplying the anterior, lateral, and inferior walls. Hence the widespread ST elevation which the computer algorithm interprets as pericarditis. If the computer can make this mistake, you know it can make much less egregious mistakes (and I’ll assure you that it does).
Therefore, you must learn to read the ECG yourself.
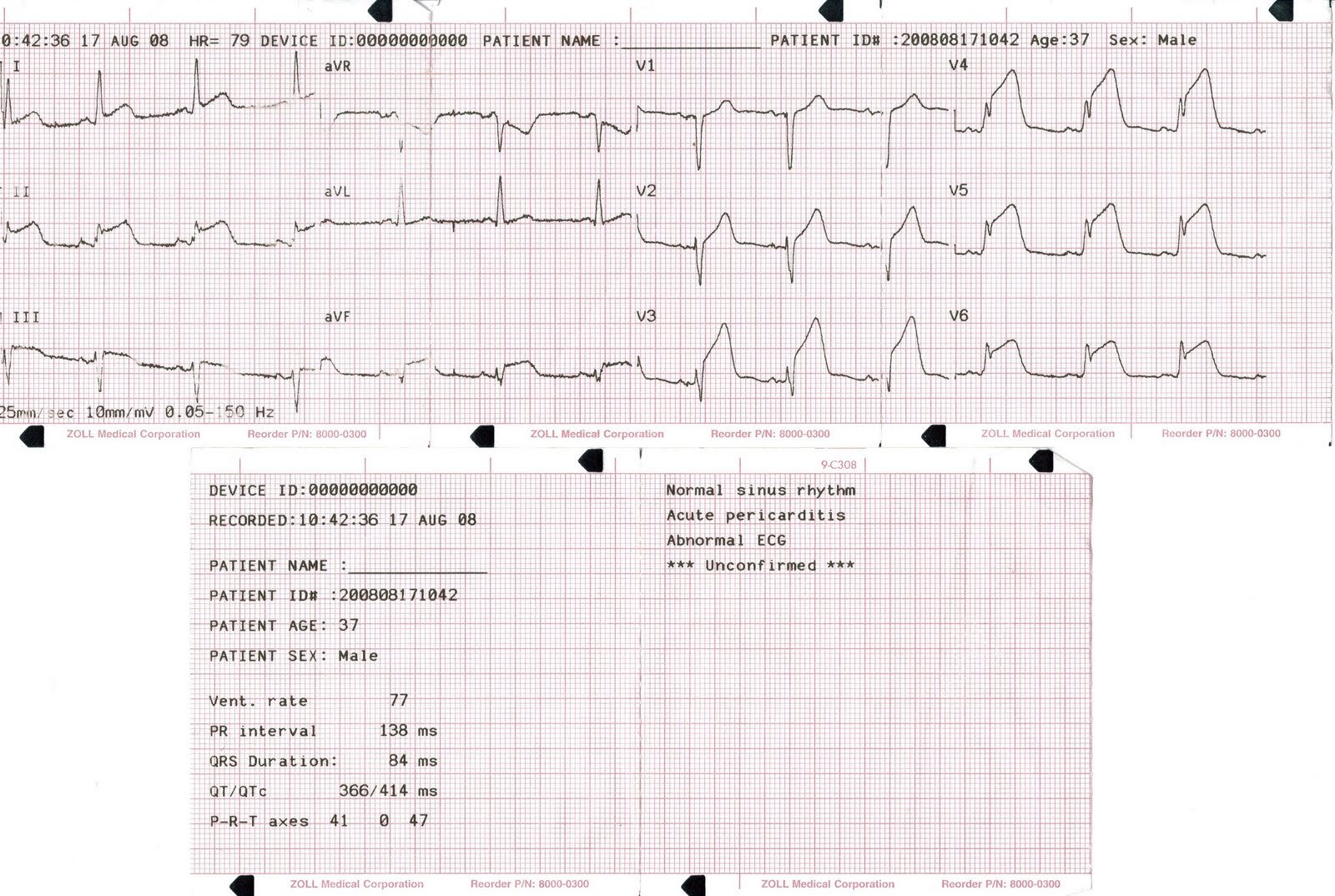
Comments indicate that I need to explain this better: The ECG represents anterior STEMI, and not pericarditis, because 1) the ST elevation is in right precordial leads (V1-V3) as well as left (V4-V6) [pericarditis has more in the inferior and lateral leads and often looks like an inferolateral STEMI] 2) unlike pericarditis, the T waves are “hyperacute”, with straight ST segments; they look wide and bulky 3) there is very poor R wave progression, 4) there is “terminal QRS distortion“, meaning the S-wave is obliterated in many leads, particulary V4-V6, and 5) the QT is long. All of these favor acute STEMI over pericarditis.