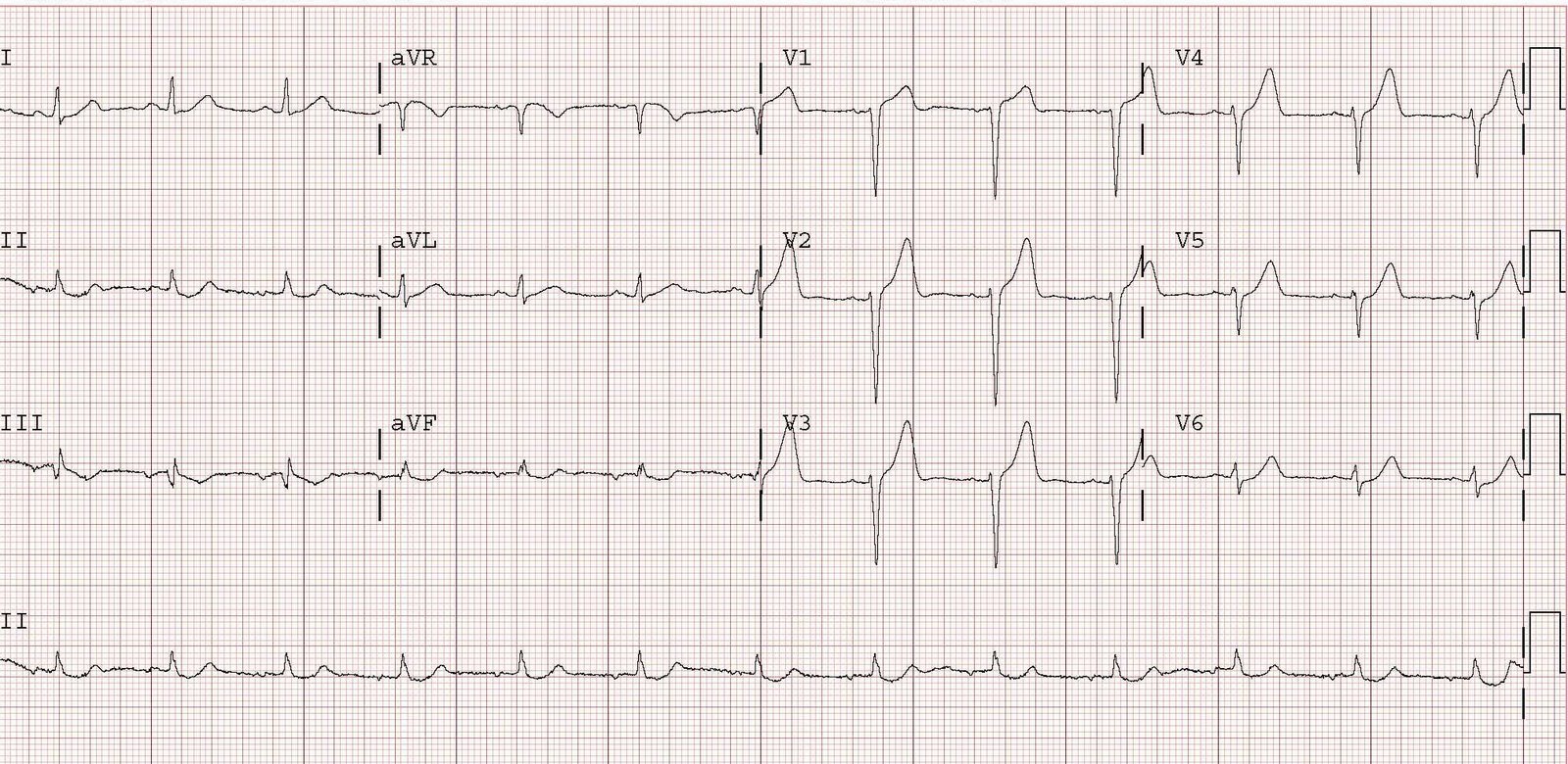
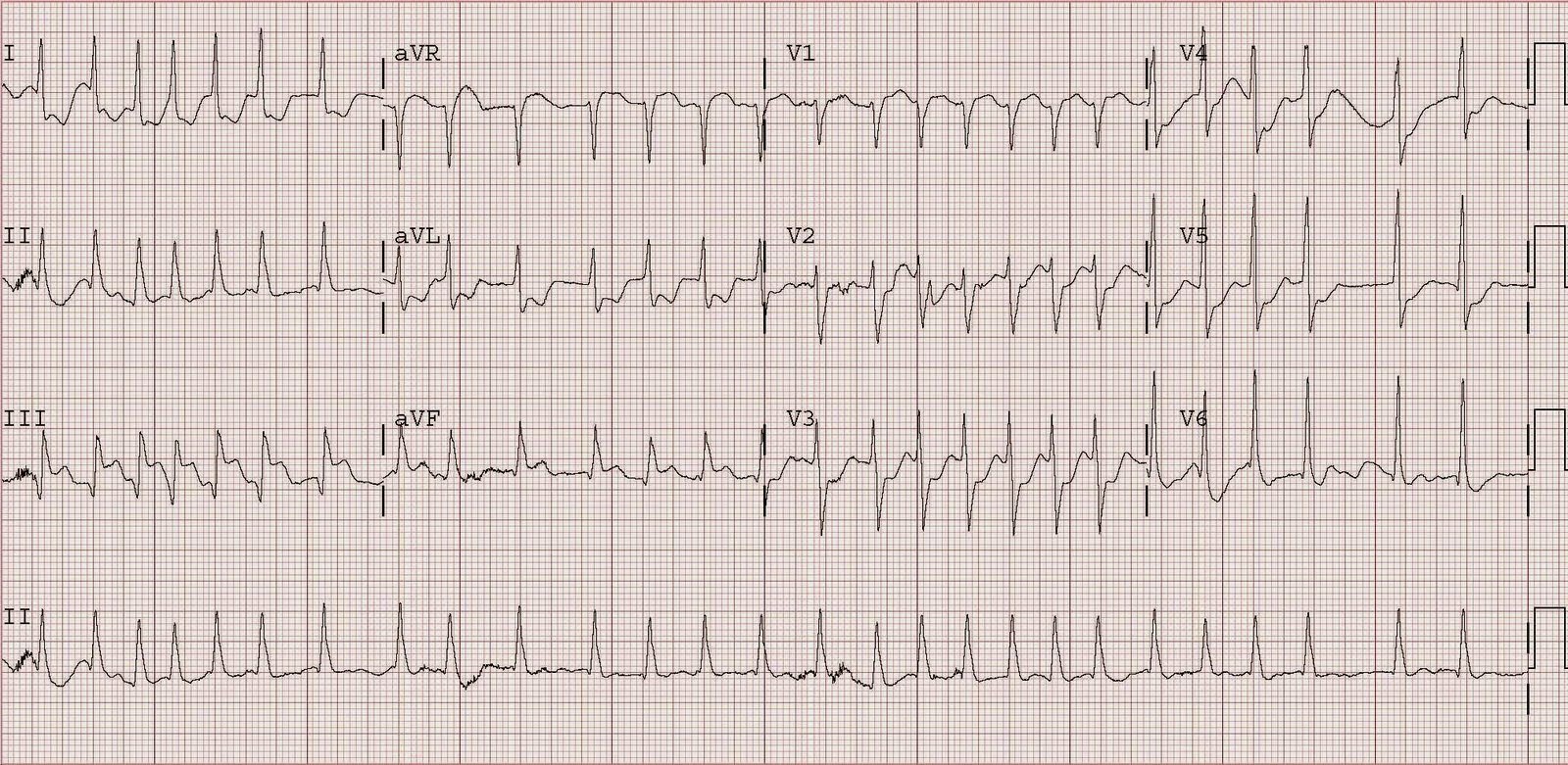
This elderly woman presented hypotensive, pale, and tachycardic. Here is the initial ECG.
 |
|
|
Did we activate the cath lab? No. We looked at the whole patient, not just the ECG. We suspected GI bleed and this was confirmed with blood on rectal exam. An ultrasound of the inferior vena cava confirmed that it was flat (low central venous pressure). Had this been a primary cardiac event, the CVP would be high and the IVC distended, and the patient might have also been in pulmonary edema.
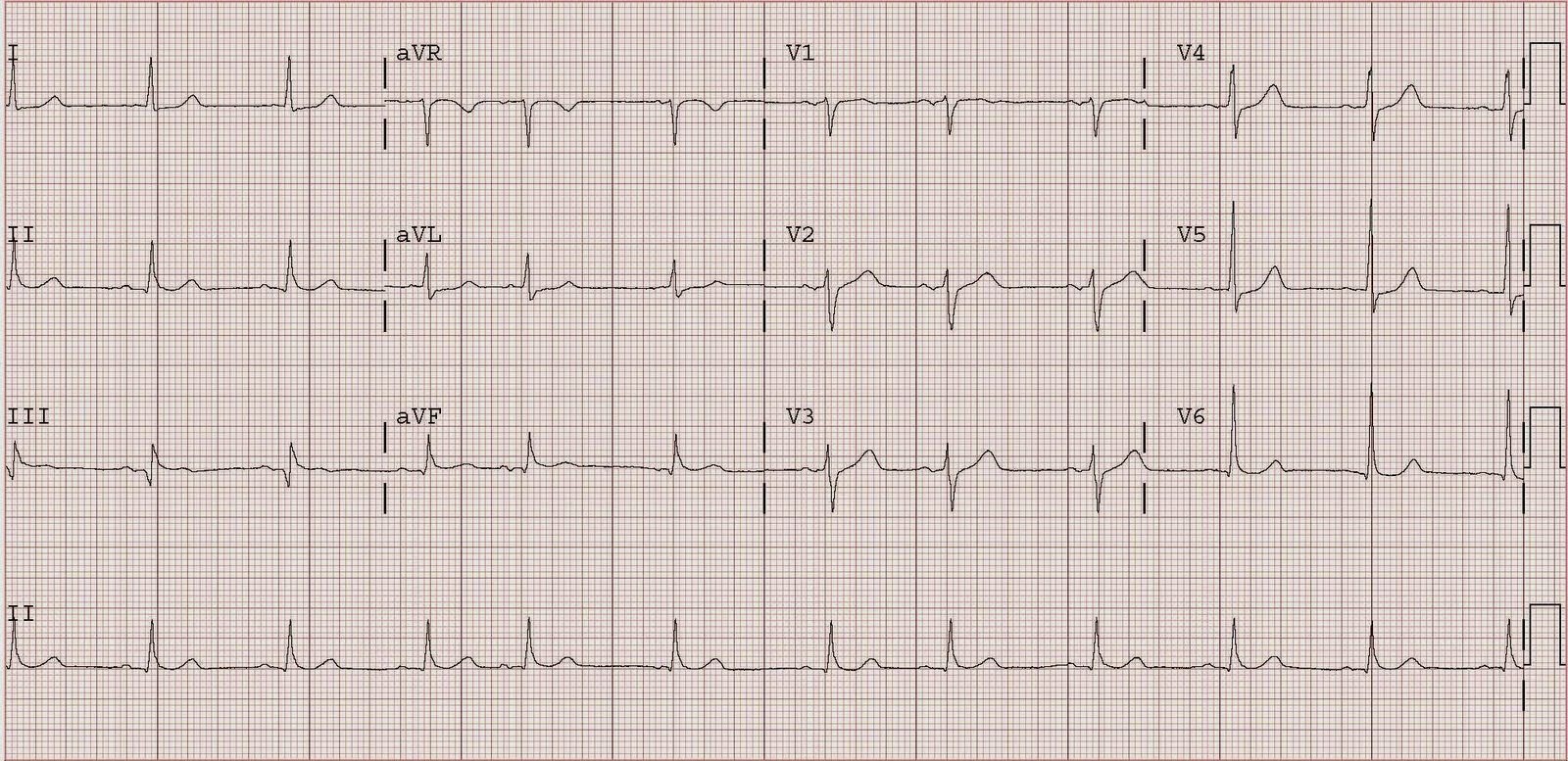
She was given blood and fluids until the bedside ultrasound showed good central venous pressure (distended inferior vena cava), but she remained hypotensive, tachycardic, and the ST elevation did not resolve. Thus, we electrically cardioverted her at 200J biphasic, but this was unsuccessful x 3. We infused amiodarone 300 mg IV, but with no improvement, and a subsequent cardioversion was again unsuccessful. We then loaded her with 500 mcg/kg of esmolol and started her on a 50 mcg/kg/min drip, after which a fifth cardioversion was successful, and resulted in the second ECG shown here:
 |
|
|
Troponin peaked at 19, and there was a subsequent inferior wall motion abnormality. A stress sestamibi showed no inducible ischemia, so no cath was done. Whether there was thrombus in the infarct-related artery, or whether this was only demand ischemia (Type II MI) is uncertain. Nevertheless, it is wise to convert atrial fibrillation with a rapid response when the patient is unstable; any injury pattern on the ECG constitutes instability.
Though demand ischemia usually shows as ST depression (or nonspecific findings) on the ECG, it may occasionally present with injury (ST elevation).