This 40-something presented with hypoxia, BP 60/30, pulse 195, and Temp of 40 C.
He had what appeared to be SVT on the monitor.
Here is his 12-lead:
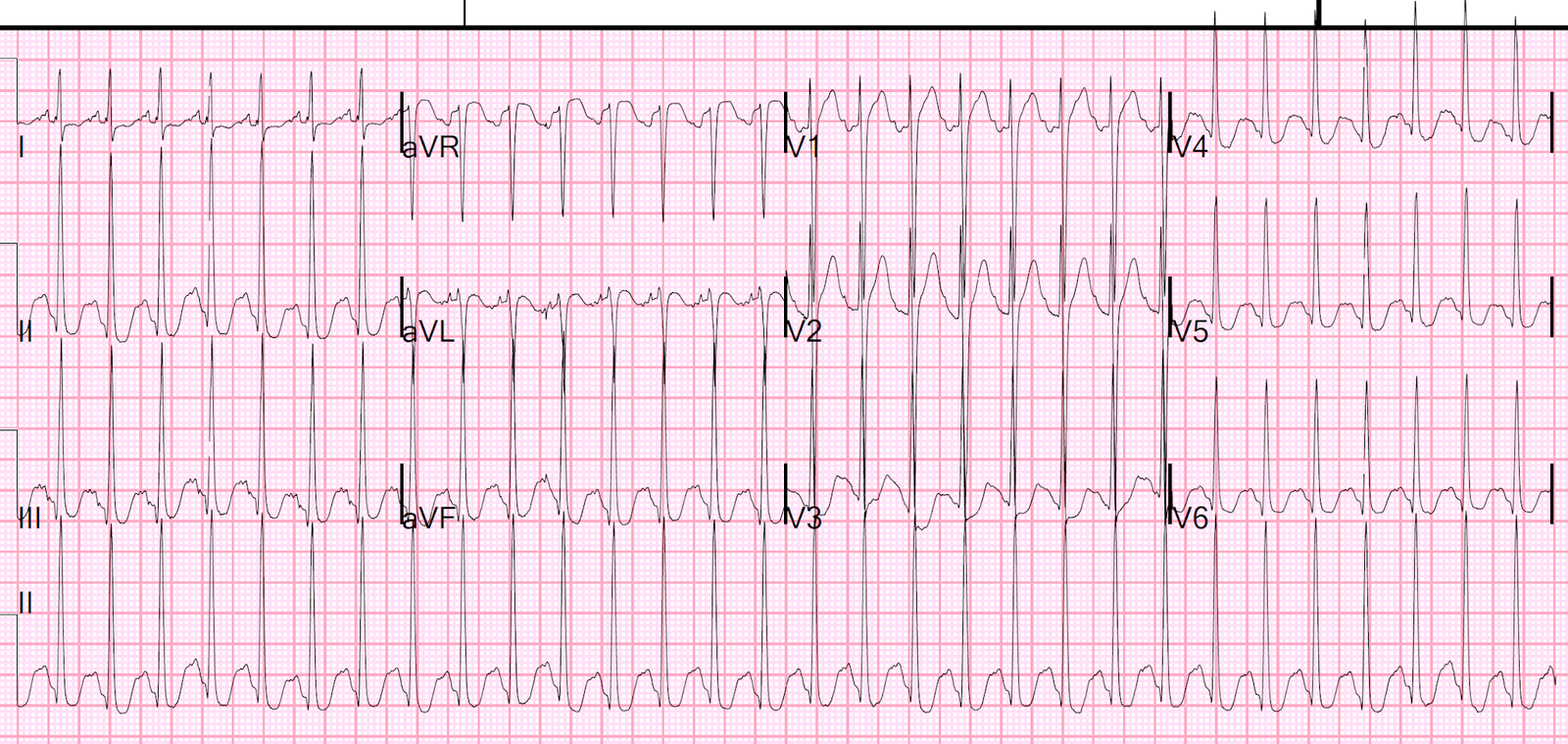
Narrow complex tachycardia at a rate of 184.
This was interpreted by the computer and the over-reading physician as “SVT”
While it is SVT, the supraventricular part is sinus. Usually when we say SVT, we are referring to a reentrant rhythm. This is why I prefer the term PSVT (Paroxysmal SVT), to distinguish sinus or other automatic SVT from re-entrant SVT.
First, when there are generators of sinus tachycardia, such as hypoxia, fever, and hypotension, sinus tachycardia should be strongly suspected.
And, indeed, if you look closely, there are clear P-waves. This is most easily seen in lead V1, where there is an “up-down” wave just before the QRS. But you can also see it in many other leads.
See magnified image of Up-down V1 P-wave here:

You can also confirm that the P-wave in V1 is simultaneous with an apparent P-wave in lead II across the bottom:

Other ways to suspect and/or confirm sinus tach vs. SVT:
1. The original heart rate was 195 (measured by the palpated pulse or the continuous monitor) but the heart rate on the ECG is 184.
Re-entrant rhythms do not change rate gradually. They are constant, or nearly so (until they break) because the re-entry circuit has a fixed rate.
The sinus node, on the other hand, is an automatic rhythm, and thus its rate varies gradually and is affected by many many factors, including catecholamines, oxygenation, hemoglobin, volume status, random variation, and many more, and varies with interventions such as oxygen, fluids, and much more many more.
2. One could apply Lewis leads. These would exaggerate the P-wave amplitude. Use the monitor, not the 12-lead ECG, and follow these instructions: https://emcrit.org/emcrit/lewis-lead/
Other cases:
A Relatively Narrow Complex Tachycardia at a Rate of 180.
Heart rate of 230 beats per minute
See here for many uses of Lewis Leads: