An elderly woman with a h/o myocardial infarction presented with 2 hours of burning substernal chest pain.
Here is her ECG:
 |
| Is there an OMI?
What is the best next strategy to assess for OMI? |
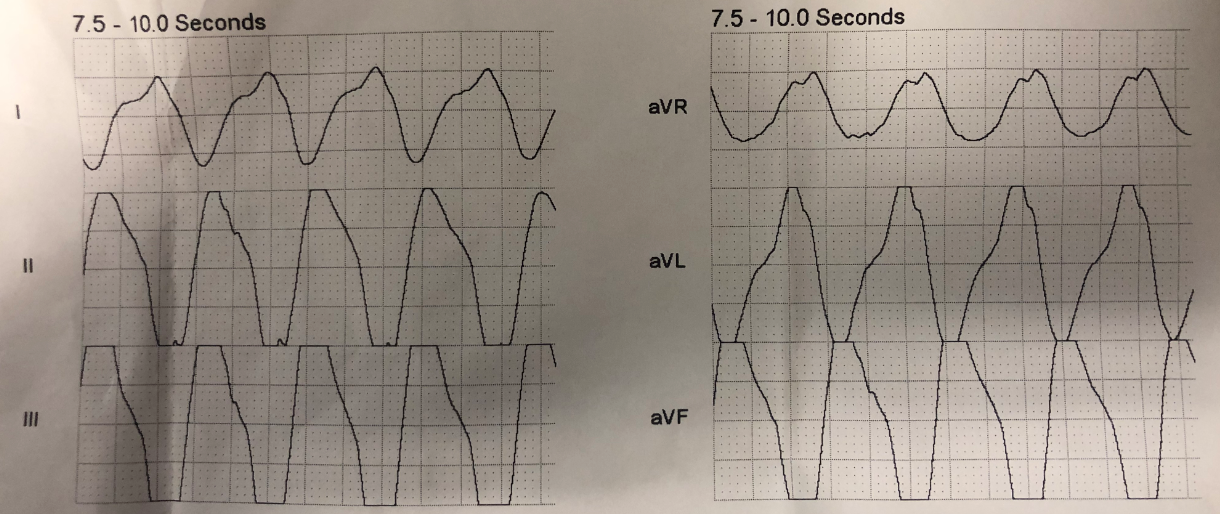
ECG description:
There is sinus rhythm. There are well-formed Q-waves in inferior leads, with some minimal ST Elevation, and reciprocal ST depression in aVL. The STE with STD in aVL is typical of inferior OMI, right?
Except for the well-formed Q-waves, which suggest an old inferior MI.
There is also an early R/S transition in precordial leads, with a large R-wave in V2. This suggests previous posterior MI as well. (Bayes de Luna would say “lateral MI”)
There are also Q-waves (qR-waves) in V3-V6 of old anterior MI.
This ECG is classic for old inferior MI with persistent ST elevation. Why? Because of very well formed Q-waves, and h/o MI.
Differentiate acute inferior MI from old inferior MI
There is no very good way to differentiate inferior acute OMI with Q-waves from old inferior MI with persistent ST Elevation. They can look remarkably similar, and so looking for old ECGs and other historical information is key.
On the other hand, anterior aneurysm (persistent STE after old MI) can be fairly reliably distinguished by the T/QRS ratio.
See this case:
Subtle Anterior STEMI Superimposed on Anterior LV Aneurysm Morphology
And many more:
https://drsmithsecgblog.com/search?q=T%2FQRS+ratio+aneurysm
So what is the Plan??
Look for an old ECG and previous echocardiogram.
Indeed, previous ECGs looked the same and the patient had inferoposterior akinesis on previous echo.
The pain resolved on its own and the patient ruled out for MI by troponin.
It is still possible that the patient had unstable angina. However, the point is that if she did have acute ischemia, it is not manifesting on the ECG. Only old infarction is manifesting.
Anyone with coronary disease and substernal chest pain, even with a normal ECG, has a high likelihood of ACS (MI or unstable angina) and should be managed as such.
Look what happens when you do not take clinical unstable angina seriously:
Beware crescendo angina in patient with known CAD
Here is another inferoposterior true aneurysm, reprinted from my book:
 |
| Notice it looks like an acute inferoposterior OMI, except for the well formed inferior Q-waves. There are no large R-waves in V1-V3 (which would be expected with old posterior MI). This is because there was also an old anterior MI with anterior Q-waves. This was proven on echo (diastolic dyskinesis) and the patient ruled out for MI by troponins. |
Here are 3 previous posts on the topic of inferior aneurysm:
Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
Pulmonary Edema, Hypertension, and ST Elevation 2 Days After Stenting for Inferior STEMI
Tachycardia must make you doubt an ACS or STEMI diagnosis; put it all in clinical context
![]()
===================================
MY Comment by KEN GRAUER, MD (11/29/2019):
===================================
Straightforward, but very important case by Dr. Smith regarding making distinction between acute vs old infarction. This task was especially challenging in this case — because this elderly woman with a history of prior MI presented with new-onset (began 2 hours earlier) substernal chest pain. I’ll add the following thoughts to commentary by Dr. Smith.
- For clarity — I’ve reproduced and labeled the ECG in this case in Figure-1.
 |
| Figure-1: The initial ED ECG in this case (See text). |
My Thoughts on ECG #1:
- Dating an infarction by ECG is an imperfect science — with heavy dependence on History (ie, “When did your chest pain begin?” ). That said — not all patients with acute MI have chest pain — and even when they do, there is often not a reliable history as to when the symptoms began. And then, many patients who present with chest discomfort — end up not having acute infarction …
- Realistically, often the “best” we can do from interpreting an ECG is to say that ECG changes look “ACUTE” (ie, just happened, or probably happened no more than a few hours earlier) — vs “OLD” (happened at some point in the past = more than a few days ago, up until months or years previously) — vs “SUBACUTE” or “RECENT” (ie, happened at some point in time between our definition of “acute” or “old” ). That said, there is an additional category — which is, that there may have been prior infarction and then superimposed on an old MI, is a new acute event. That is the situation suggested by the ECG in this case.
- Independent of this patient’s history — We KNOW there has been previous inferior MI in ECG #1. Not only are each of the inferior Q waves deep (especially considering the modest height of R waves in these leads) — but in addition, these Q waves are wide (especially in leads III and aVF) — and, there is marked fragmentation (notching) in each of these 3 inferior leads. While any of these 3 features alone (ie, increased depth of Q waves — or — increased width of Q waves — or — definite fragmentation of the QRS), if seen in one or more of the 3 inferior leads, increases the likelihood that inferior Q waves represent prior infarction — seeing all 3 of these features in each of the 3 inferior leads (as we do in this case) — makes it a virtual certainty that there has been prior inferior MI.
- There are Q waves in leads V3-thru-V6 (Be sure you note that the initial deflection in lead V3 is a small-but-definitely-present q wave). These Q waves in the anterolateral chest leads are not normal because: i) Depth of the Q wave in lead V6 is clearly disproportionately deeper-than-should-be-expected for a “normal septal q wave”, especially given the modest R wave amplitude in this lead; ii) While possible for “normal septal q waves” to extend as far over as lead V4 — they should not be seen in lead V3 — especially given the relatively tall R wave that we see in lead V3; and, iii) There is marked fragmentation of the QRS complex in leads V4, V5 and V6. These points taken together suggest that the precordial Q waves we see in leads V4-V6 are the result of prior lateral (or antero-lateral) infarction.
- As per Dr. Smith, the finding of early transition (ie, R=S already by lead V2, with persistence of surprisingly tall R wave amplitude in neighboring lead V3) strongly suggests prior posterior MI, especially given the virtual certainty of prior inferior MI (ie, there is usually a common blood supply to the inferior and posterior walls).
Findings in ECG #1 that suggest an acute event may be occurring include:
- Slight-but-real ST elevation in the inferior and lateral precordial leads.
- Extra peaking (almost pointed) T waves in each of the 3 inferior leads.
- Mirror-image oppositely directed T wave inversion in lead aVL (with lead I also showing a smaller amount of similarly-shaped T wave inversion).
On the other hand — ECG findings suggesting that ECG #1 does not represent an ongoing acute event include:
- Well-established Q waves in the inferior and lateral precordial leads, in association with marked fragmentation in multiple QRS complexes (ie, fragmentation is often a longterm sign that indicates infarction or scarring has occurred at some point in the past).
- Distinct straightening of the ST segment (prior to the onset of the T wave) that is seen in multiple leads (See straightened horizontal, or almost horizontal RED lines in ECG #1).
- Lack of ST segment depression in those leads with T wave inversion (which are leads I and aVL).
- Lack of any ST depression at all in leads V1, V2 and V3 (ST depression in at least 2 of these leads is almost invariably present when posterior infarction is recent).
BOTTOM LINE: I would have guessed that the findings in ECG #1 were not acute — but as per Dr. Smith, I was not at all certain. The inferior lead T wave peaking (with oppositely-directed T wave inversion in lead aVL) could have been an acute change superimposed on prior inferior MI …
- Finding a prior ECG on this patient, as well as a prior Echo report turned out to be invaluable for confirming that ECG #1 showed no acute changes.
- FINAL POINT: Ideally, you will be able to find not only a prior ECG on your patient — but also enough clinical information to ensure that the previous ECG you located reflects a true “baseline” tracing (and that this previous ECG was not obtained at the time of a prior recurrence of an acute event)!
Our THANKS to Dr. Smith for presenting this case!
![]()