This is a 58 year old woman with a history of inferior MI. She has had a week of intermittent substernal chest heaviness associated with SOB. Because it came again and lasted for one hour, she called 911. The medics recorded a 12-lead, then gave her aspirin and nitro, and her pain resolved completely. It seems the physicians caring for her did not see this ECG, so I am not showing it first. On arrival in the ED around midnight, she was pain free and had this ECG recorded:
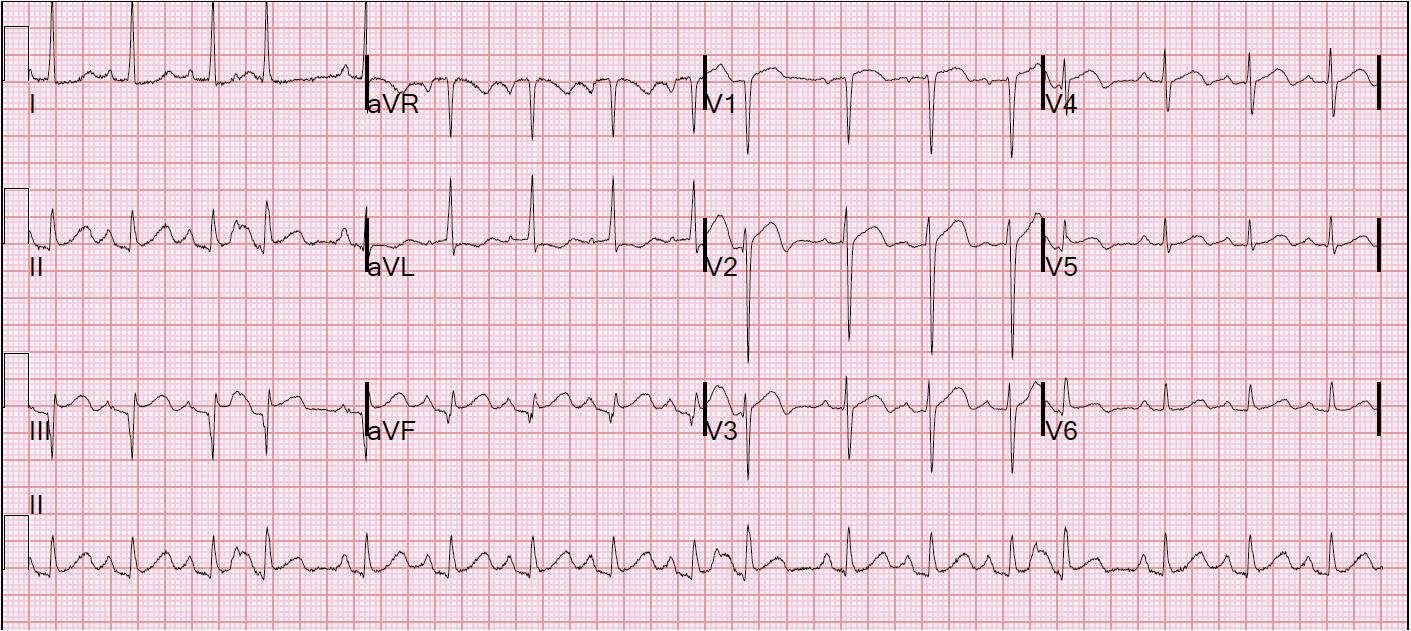 |
| First ED ECG. Sinus rhythm with a couple of PACs. Heart rate is close to 100, so one must entertain hemodynamic etiologies of chest pain, such as pulmonary embolism. There are Q-waves with minimal ST elevation in inferior leads and reciprocal ST depression in aVL, not significantly changed from baseline (ECG below). There is also minimal ST elevation in V1 and V2 with the beginnings of T-wave inversion suggestive of anterior NSTEMI (“Wellens’ syndrome”). |
The first ECG is substantially different from the previous ECG 3 years prior:
 |
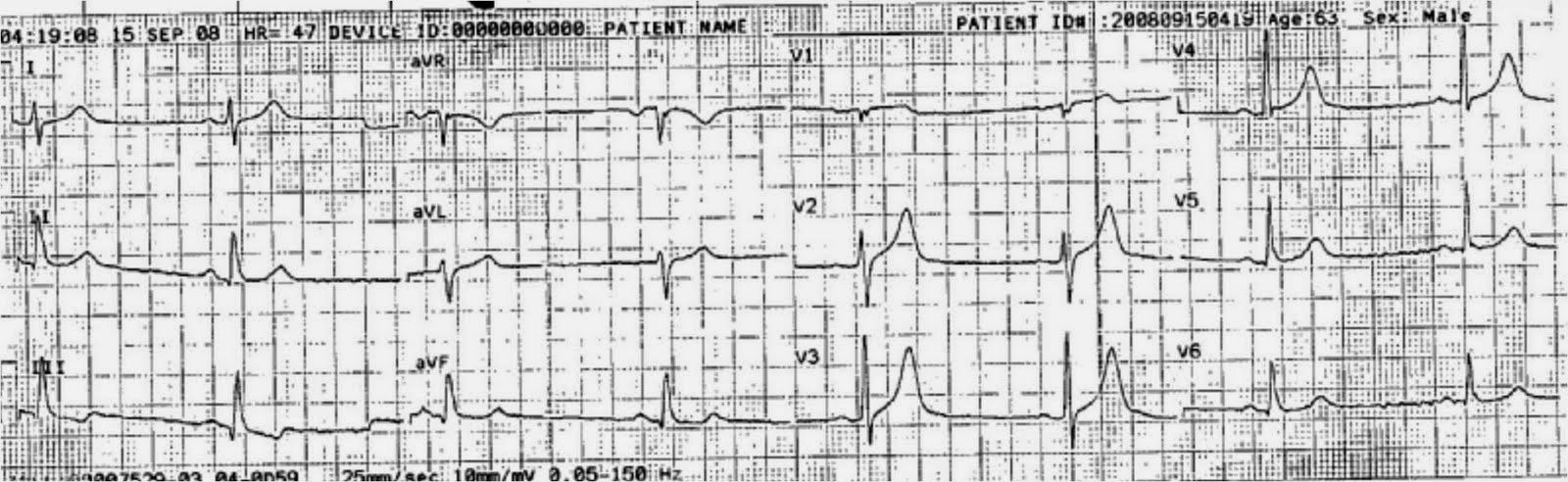
| Previous ECG from 3 years prior shows old inferior MI and baseline precordial ST elevation of early repolarization. There is upward concavity and normally upright T-waves. |
Prehospital ECG during chest pain, before nitro and aspirin.
 |
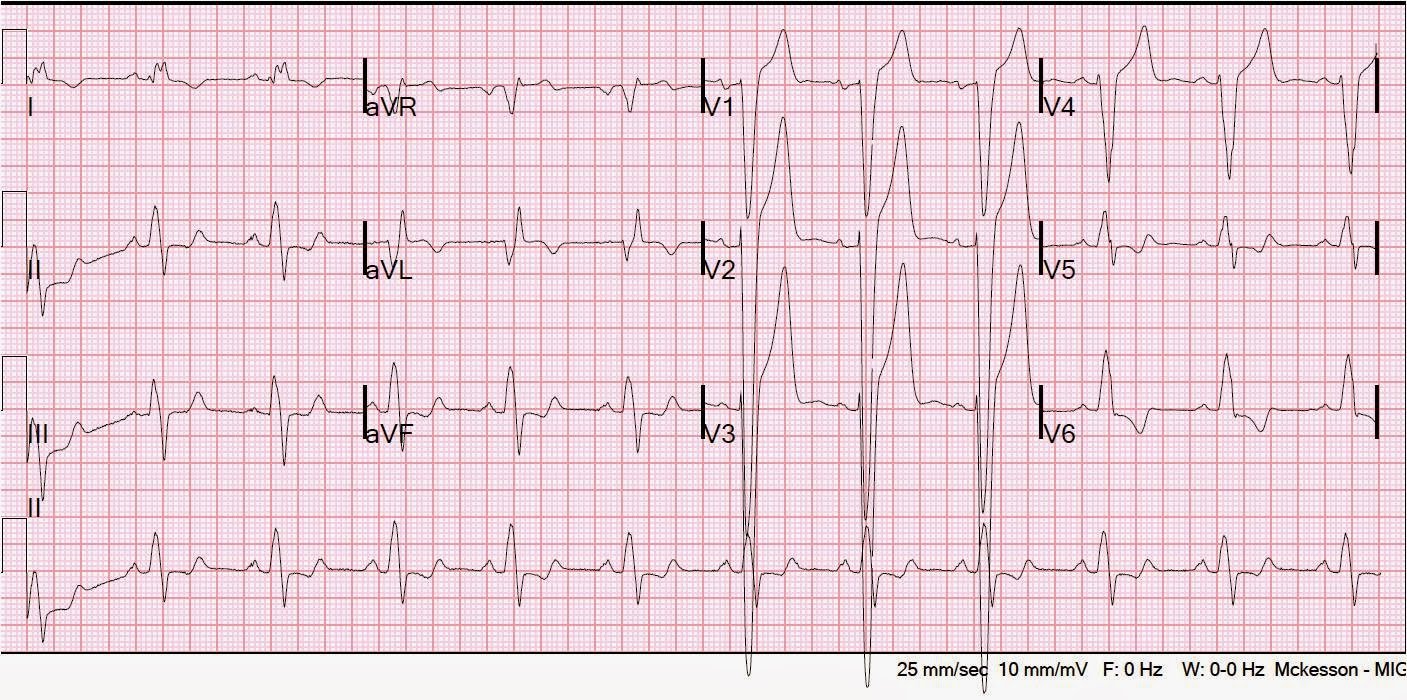
| There is ST elevation and a large upright T-wave in V1, different from the baseline T-wave. The LAD may well have been occluded during this recording. |
ECG 2.5 hours after presentation, no therapy other than aspirin:
 |
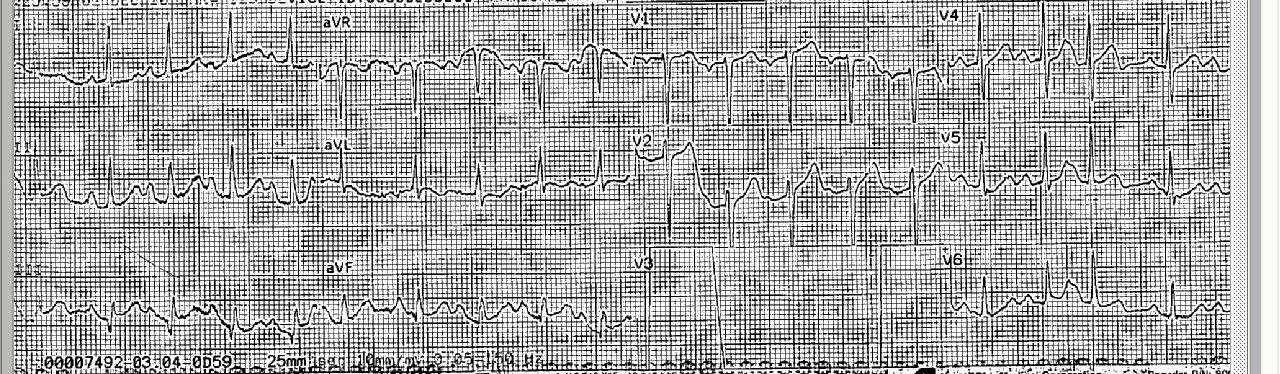
| The terminal T-wave invesions are still present and perhaps more noticeable. |
At this point, the troponin returned at 0.14 ng/ml (limit of detection: 0.012; 99% reference value: 0.034, so this is a “positive”).
Here is a third ED ECG at 6 hours:
 |
| The terminal T-wave inversions in V2-V4 are more obvious. This is typical of Wellens’ pattern A. |
The K was also 2.9 mEq/L, but this does not account for the ECG findings. The patient had a negative PE workup and was admitted to the hospital. She had a rise and fall of troponin, with a peak at 0.358 ng/ml. She went for an angiogram the next AM; it showed mid-LAD culprit lesion with 95% stenosis and was stented.
This is after LAD stenting:
 |
| After stenting, there was another rise and fall of troponin. Now the Pattern A Wellens’ waves are very well developed. |
T-wave inversion in LAD ACS:
Wellens’ syndrome is chest pain that is relieved with terminal T-wave inversion on the initial, pain-free, ECG. There is preservation of R-waves, and there is evolution to deeper T-wave inversion (Wellens’ Pattern B). It is due to brief LAD occlusion with reperfusion. This last evolution (Pattern B) did not occur in this case.
See here for a series of classic Wellens’ evolution over 26 hours.