See this post for a wide complex that reveals the MI.
Case:
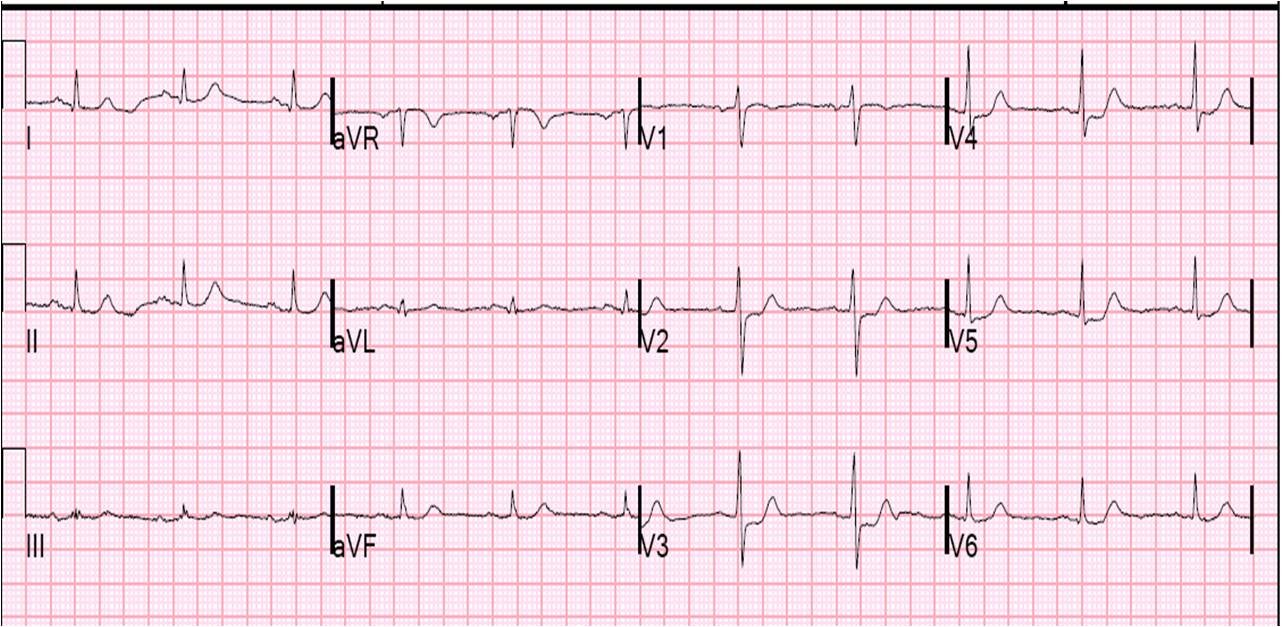
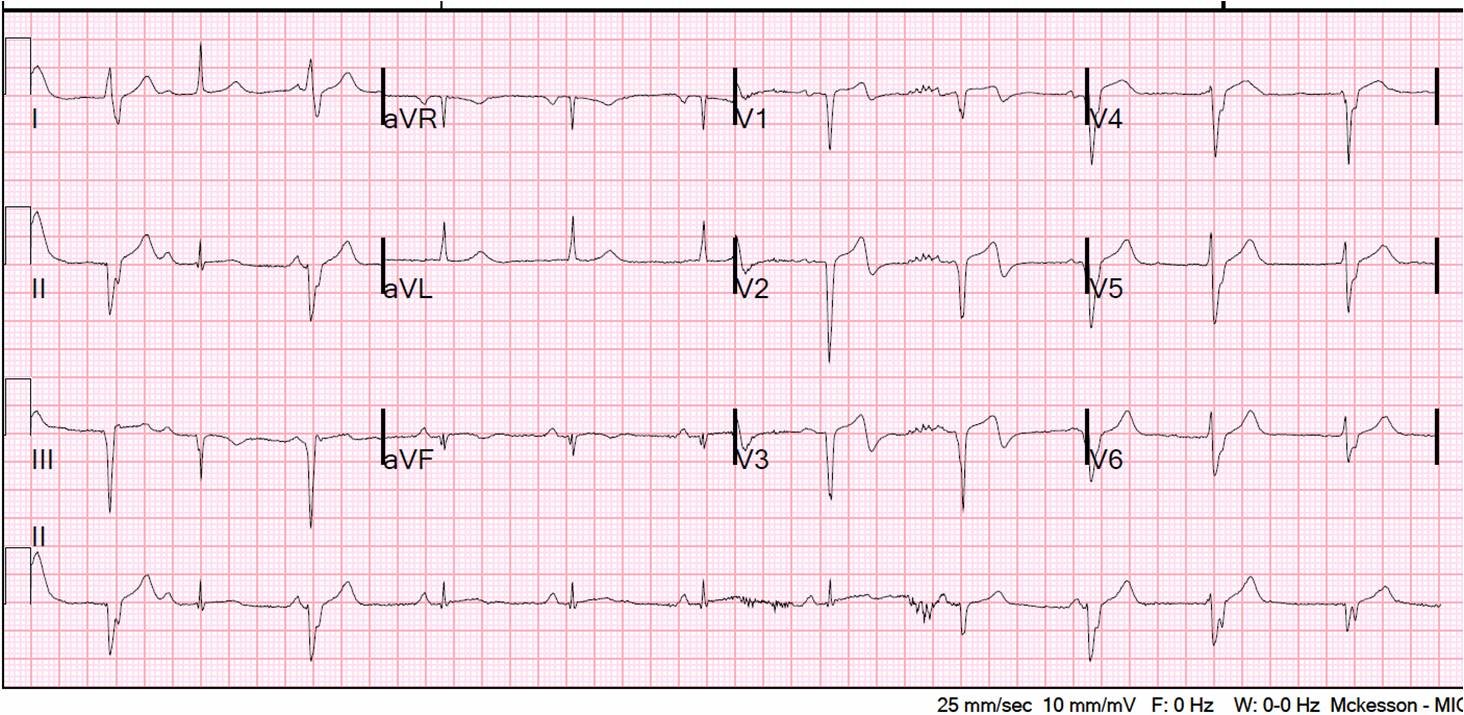
This 46 yo male with no h/o MI or coronary disease presented with 2 days of palpitations, nausea and dizziness and intermittent chest pain that started while walking. The chest pain was never prolonged and constant. Here is his initial ECG (816 AM):
 |
| There is occasional sinus rhythm (beats 2, 7, and 13) with narrow complex and the remainder have an uncertain origin (left bundle escape rhythm?) with RBBB morphology. Leads V1-V3 have no complex that is narrow. Narrow complexes can be seen in other leads and V4 is most remarkable, with minimal if any R-wave, then ST elevation and biphasic T (up then down). This is highly suspicious for MI. |
V1-V3 have RBBB morphology, but the initial r of the rSR’ is replaced by a Q-wave. V3 has an RBBB pattern with ST elevation. There is 1 mm of ST elevation in V1-V3 in the presence of RBBB; this is abnormal, but when there is a Q-wave, it can be due to old MI with persistent ST elevation. ST segments in RBBB in V2 and V3 are usually negative, opposite the tall R’ wave. Any ST elevation is abnormal.
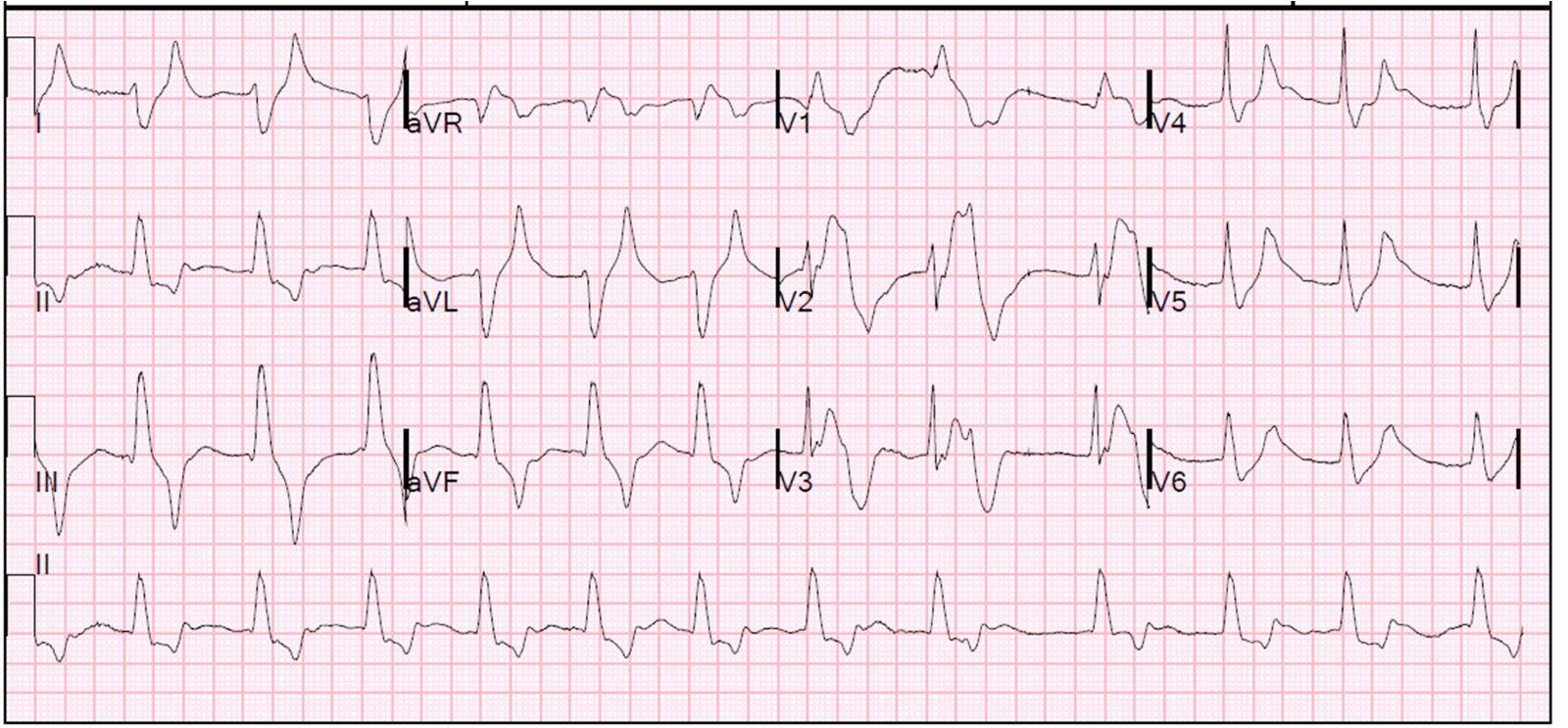
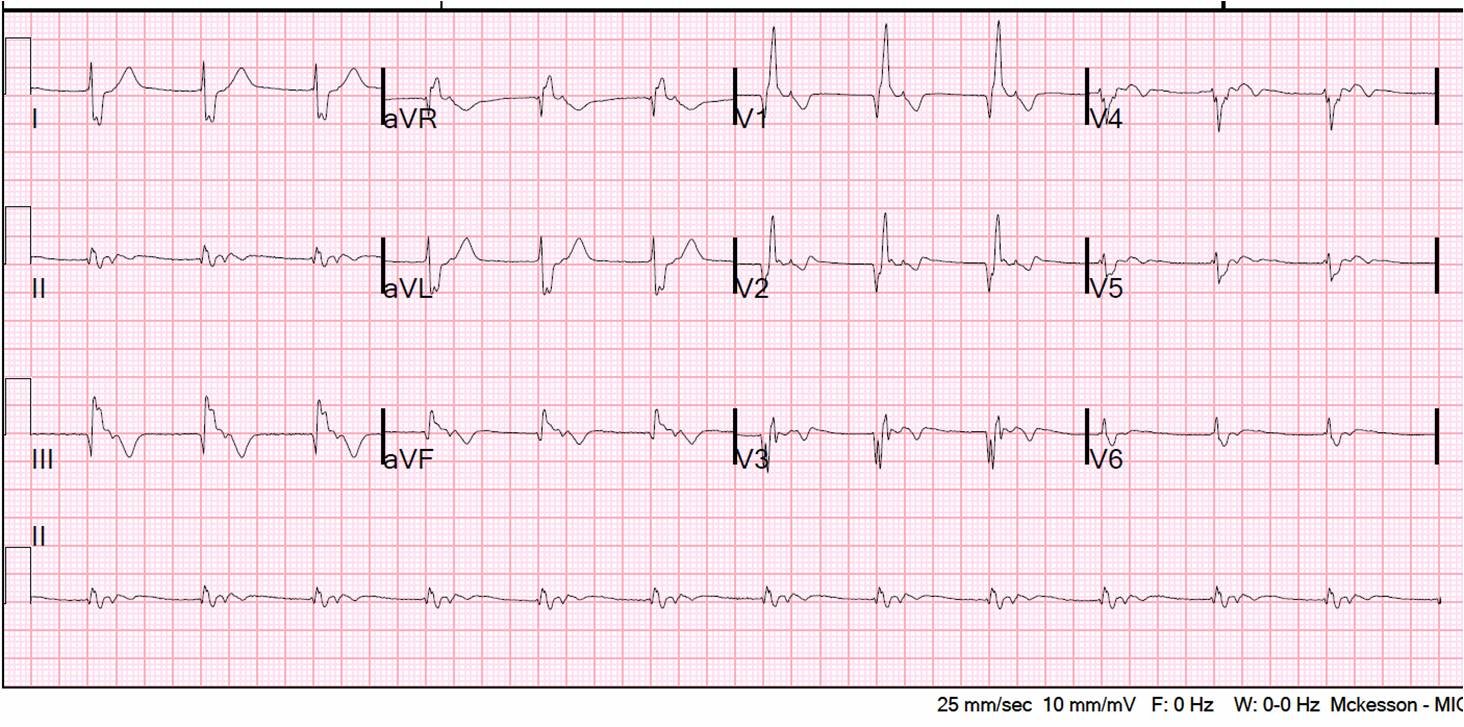
This was unrecognized, and at 941 AM another ECG was recorded:
 |
| In this recording, the 4th and 10th complexes are narrow, and the 5th and 11th appear to be fusion beats. ST elevation remains in V3 (abnormal, diagnostic of old or new MI). V4 still has biphasic T-waves. |
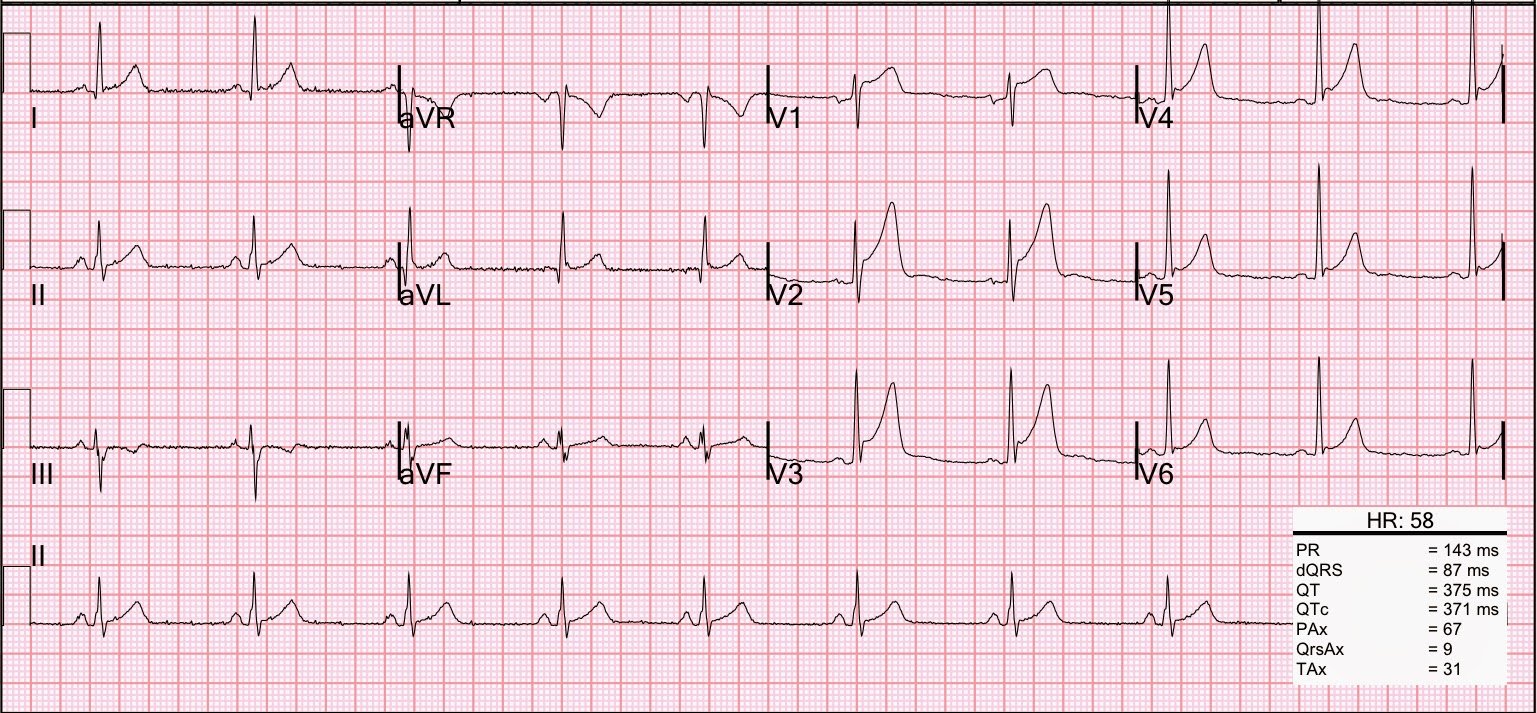
At this point, the troponin returned at 81 ng/ml and the cath lab was activated. A 70% ulcerated lesion with thrombus was found in the proximal LAD. Thrombus was suctioned and stent placed. Here is the post cath ECG:
 |
| Finally we have a QRS that is of normal duration, and it has the classic biphasic T-waves of Wellens’ syndrome, but is NOT Wellens’. Why? Because Wellens’ syndrome has preservation of R-waves. Wellens’ is a sentinel event, warning of massive MI. In this case, the massive MI has completed and there are QS-waves. |
Here are many cases discussing Wellens’ syndrome, and here is one in particular that shows the classic progression over time.
The troponin peaked at 175, there was a large anterior, septal and apical WMA with EF of 40%.
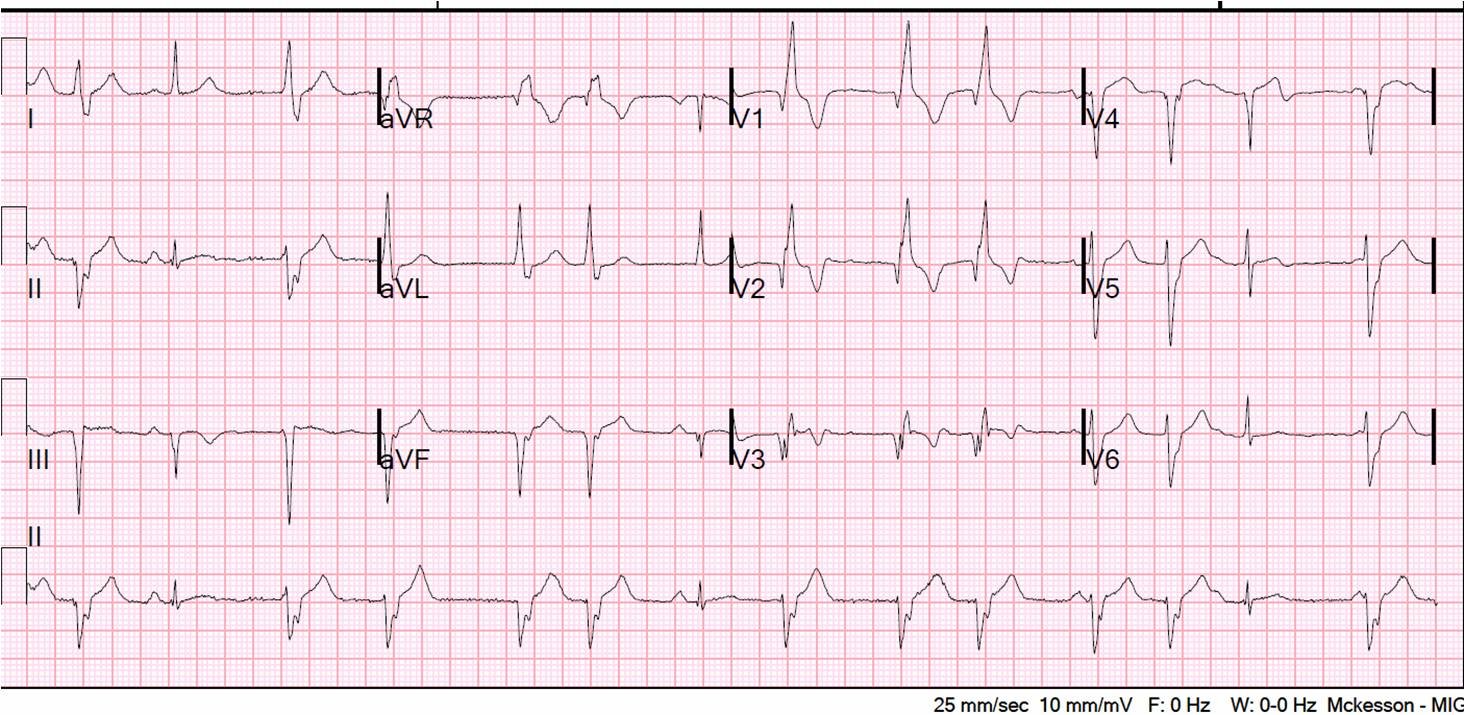
Here is a slightly later recording:
 |
| During this recording, the patient was again going in and out of RBBB (RBBB in complexes 1, 3, 9, and 10; 8 and 11 are fusion beats), and you can see how the T inversion in V4-V6 (where there are no normal complexes) is completely hidden by the RBBB morphology. RBBB has rendered the T waves upright. |
This was recorded 3 days later:
 |
| The escape rhythm with RBBB morphology remains, and all T-wave changes are obscured. Thanks to VinceD for recognizing the retrograde (inverted) p-waves buried in each RBBB complex. |
Summary:
1) For help in diagnosis, look for the complexes that have a normal QRS
2) In RBBB, any ST elevation in V1-V3 is abnormal
3) Q-waves in RBBB, with ST elevation, may be subacute MI or old MI with persistent ST elevation.