Case 1)
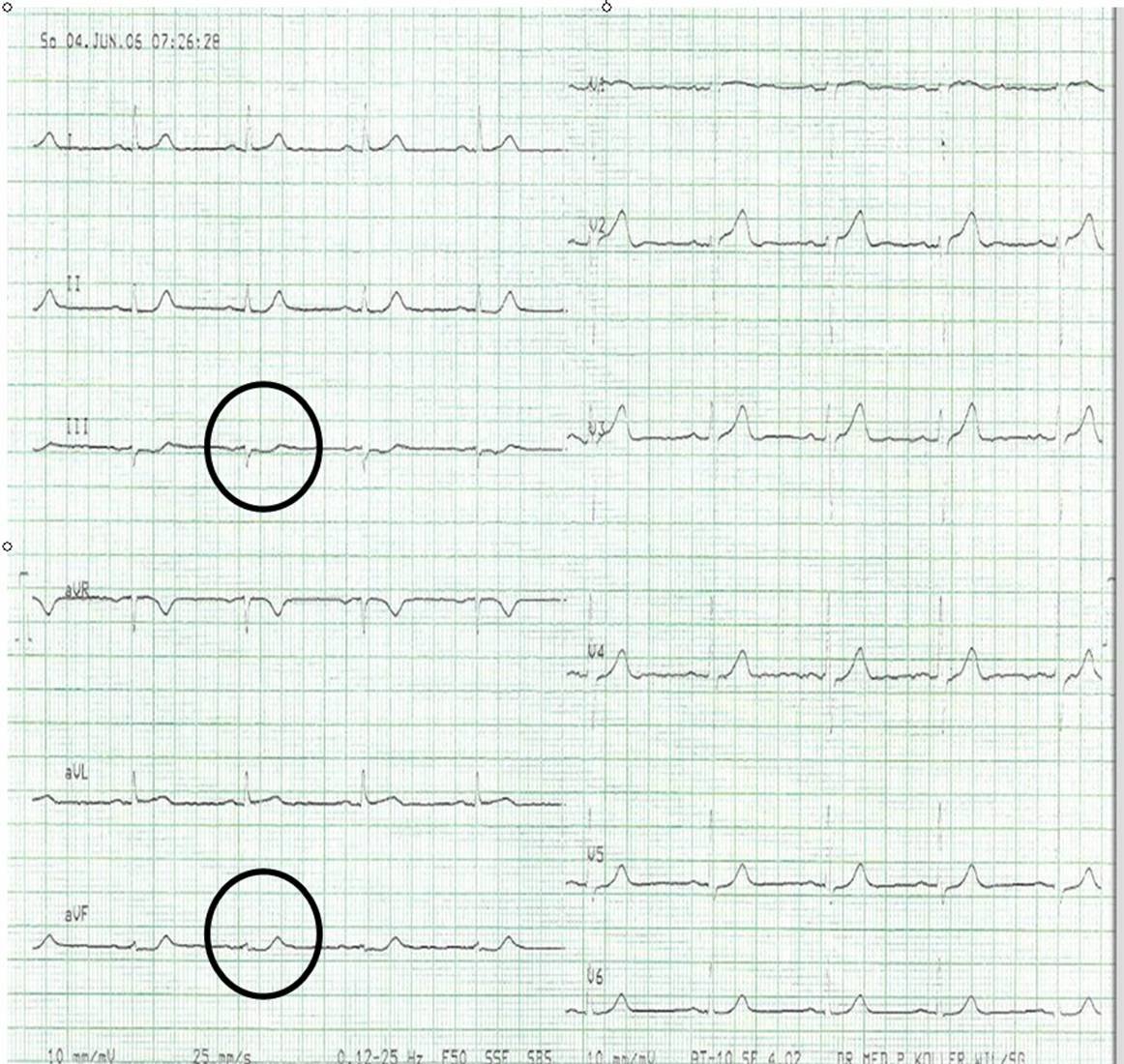
This is the initial EKG of a 60 yo male with a couple days of stuttering chest pain. He is pain free at the time of the EKG at 2100.
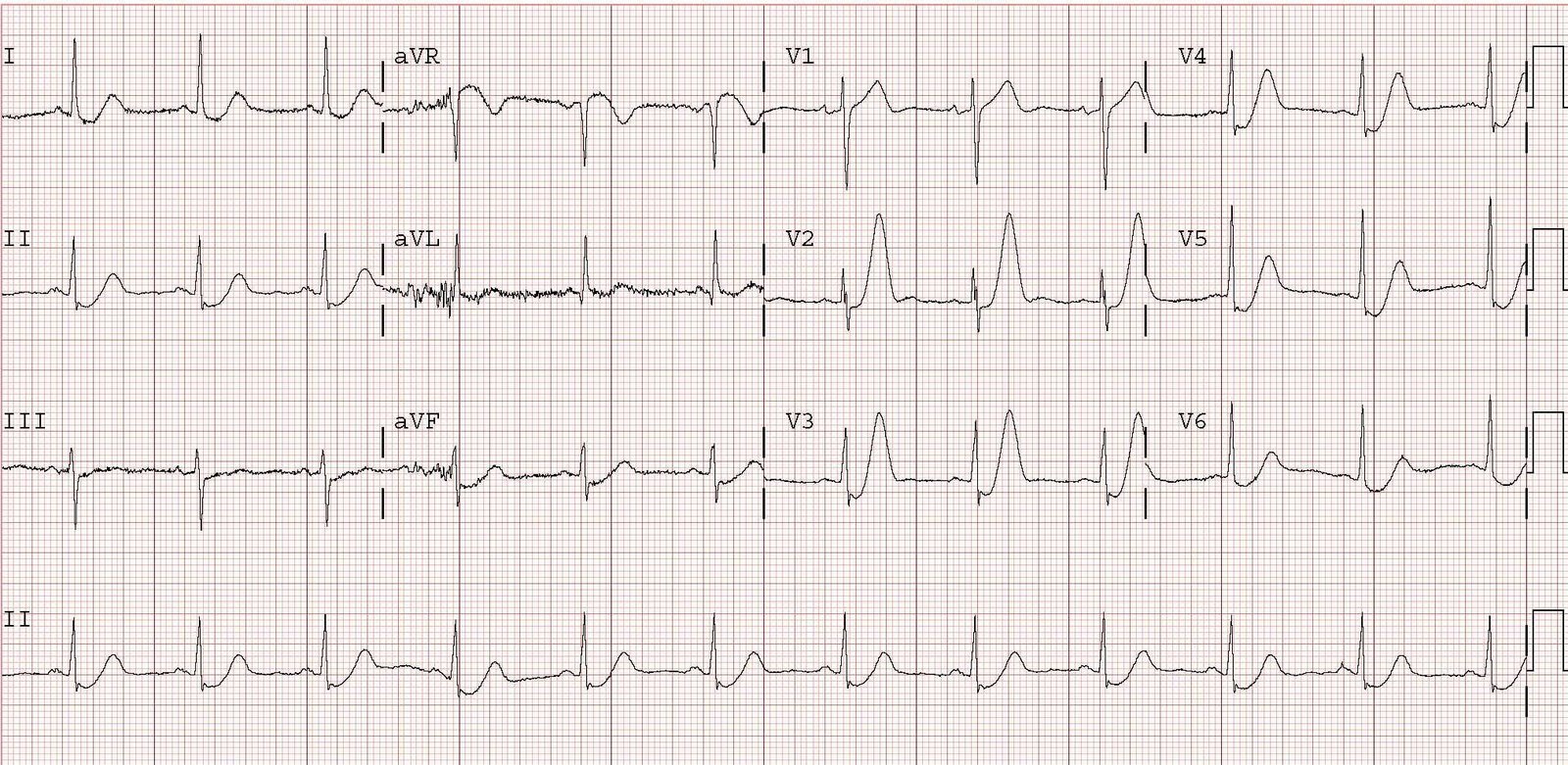
At 2140, the patient had recurrent pain, and the following EKG was recorded:

If seen alone, this EKG would not look terribly abnormal. But compared to 40 minutes prior, there is ST elevation now where there was none before, and the T-waves are much taller.
This was not appreciated by the treating physician. Even with no change in the EKG, the patient should have at least been admitted for observation. Unfortunately, the patient was discharged and suffered significant loss of the anterior wall.
Case 2)
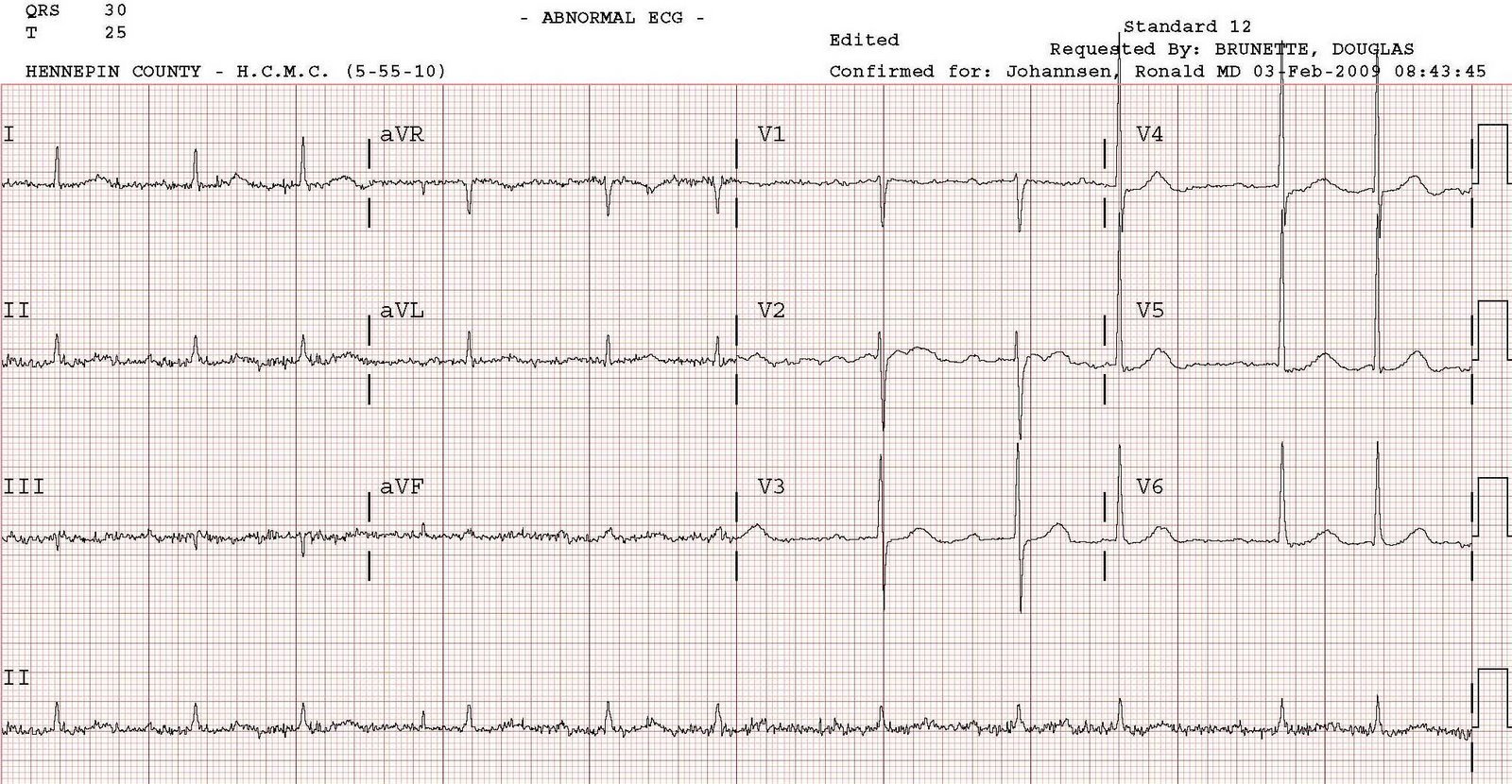
This is the initial ECG of another 60 yo man with chest pain that is now resolved.

There is left bundle branch block (LBBB) without any ST segment shift that would be suggestive of acute coronary occlusion (of LBBB with STEMI). Such shifts would be 1) concordant (same direction as QRS) ST elevation in inferior or lateral leads 2) concordant ST depression in leads V1-V3 (where the QRS is negative, ST depression would be concordant and this would be posterior STEMI) or 3) excessive ST elevation in leads with a negative QRS; excessive is greater than or equal to 20% of the preceding S-wave. This EKG has some T-waves that are suspicious for NSTEMI: in the presence of an upright QRS, these are positive T-waves in II and V6 and also biphasically positive (terminal portion upright) in I and aVL. T-waves, like the ST segment, should be opposite the QRS in LBBB without ischemia.
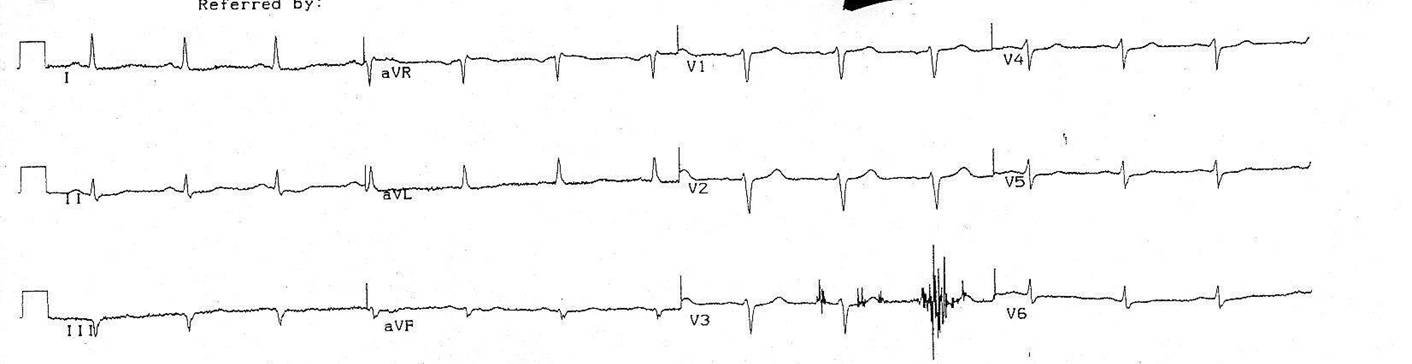
The patient was admitted to the CCU and had recurrent chest pain. The following ECG was recorded:

Now there is definite ST elevation, concordant with the QRS, in lead V5. There is also excessively discordant ST elevation in lead V2 (=25% the depth of the preceding S-wave). More importantly, these are all changes from the initial ECG. The patient’s cardiologist did not see this change and the anterior wall was lost.