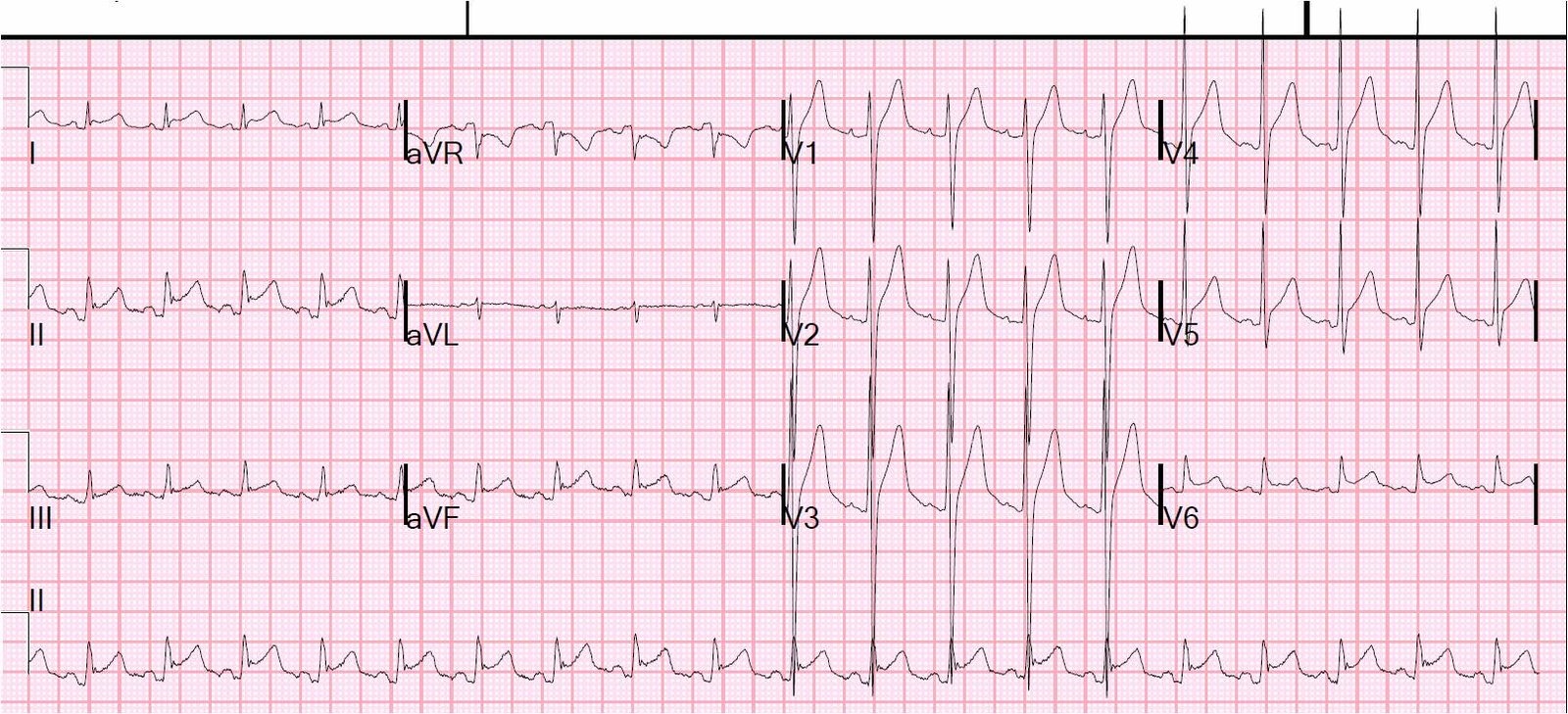
A 39 yo otherwise healthy man with no risk factors was walking at the mall when he developed chest pressure. He presented to the ED after 30 minutes, now also feeling weak. He was diaphoretic. Here was his initial ECG:
 |
| There is sinus rhythm. There is abnormal T-wave inversion in V2 (in morphology, consistent with “persistent juvenile pattern” because the R-wave is not greater than the S-wave, but this would be very unusual in a 39 yo male). There is minimal, nondiagnostic ST elevation in inferior leads without any reciprocal ST depression in aVL. There are thin and normal inferior Q-waves. Thus, there are some suspicious abnormalities, but no definite signs of ischemia. |
Because of persistent symptoms, another ECG was recorded 30 minutes later:
 |
| There is only one new finding on this ECG which suggests ischemia. It is very subtle but real. Look at lead V3, where there is now some ST depression. The previous ECG has a small amount of appropriate ST elevation in V3. Any ST depression in a young male is abnormal, especially if changed from previous. This is especially worrisome when combined with the abnormal T-wave in V2. |
Let’s look at both V3’s, magnified:
 |
| The later ECG (bottom panel) shows minimal ST depression in V3. The top shows minimal ST elevation (normal). The difference is significant and highly suggests posterior ischemia. |
This abnormality in V3 was apparently not seen by the treating MD, who is a nationally recognized expert in STEMI care (showing how difficult these diagnoses can be).
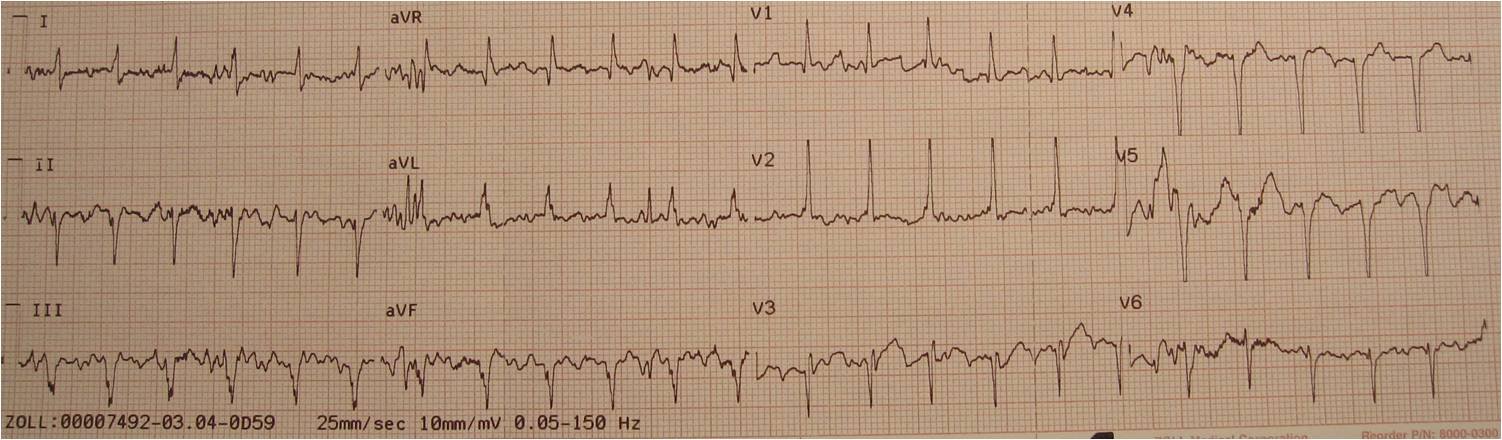
The initial troponin was negative. The patient was admitted to telemetry. At 4 AM, his second troponin returned at 1.8 ng/mL. Another ECG was recorded:
 |
| T-waves in V2 and V3 are now upright and larger, evolving. Are these posterior reperfusion T-waves? |
He went for cath at 6 AM and had on occluded OM-2 that was opened and stented. Troponin I peaked at 99 ng/mL (large MI)!
So this is a NonSTEMI, right? Technically, yes, because there is not 1 mm of STE in 2 consecutive leads. But the definition misses the point. It is a coronary occlusion with a substantial myocardial territory at risk, that showed only very subtle ST changes.
Should you activate the cath lab for this?
Not from the ECG alone. However, if you notice the ST depression, you then realize that this is ischemic chest pain, not esophageal spasm. Once you know that the chest pain is ischemic in origin, and you cannot control it medically, then you must go urgently to the cath lab.
The patient should be treated with NTG, Aspirin (and clopidogrel, if your institution allows), metoprolol, antithrombotics, and GP IIb IIIa inhibitors. If the pain persists, and the ST depression persists, then talk to your interventionalist immediately.
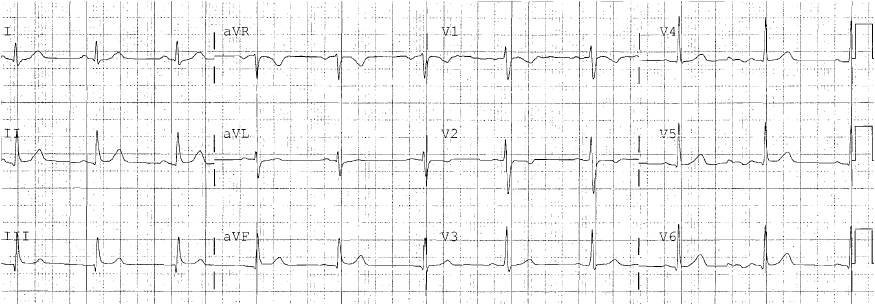
Here is the followup ECG:
 |
| The ST abnormalities have resolved. There are new inferior Q-waves diagnostic of inferior MI. The R-wave is increased in V2, consistent with MI (analog of a Q-wave). There is no apparent resolution of the minimal and non-diagnostic inferior ST elevation. |
I don’t have all the data on this case, and do not know if there is an inferior wall motion abnormality, or if this OM-2 supplied the inferior wall. It probably did, as evidenced by the Q-waves; but it is very interesting that during the acute phase, there were no diagnostic ST changes in inferior leads, and the minimal ST elevation that was present did not evolve.
Many MIs are electrocardiographically “silent,” especially when in the circumflex territory. I do wonder whether, in the studies that show this phenomenon, if an ECG expert evaluated the ECG for the subtle signs of ischemia. I suspect that many or most that are thought to be “silent” are really just “subtle.”
Here are more electrocardiographically subtle MI.